

Effects of aspirin plus extended-release dipyridamole versus clopidogrel and telmisartan on disability and cognitive function after recurrent stroke in patients with ischaemic stroke in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial: a double-blind, active and placebo-controlled study
- PMID: 18757238
- PMCID: PMC2772657
- DOI: 10.1016/S1474-4422(08)70198-4
Effects of aspirin plus extended-release dipyridamole versus clopidogrel and telmisartan on disability and cognitive function after recurrent stroke in patients with ischaemic stroke in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial: a double-blind, active and placebo-controlled study
Erratum in
- Lancet Neurol. 2008 Nov;7(11):985
Abstract
Background: The treatment of ischaemic stroke with neuroprotective drugs has been unsuccessful, and whether these compounds can be used to reduce disability after recurrent stroke is unknown. The putative neuroprotective effects of antiplatelet compounds and the angiotensin II receptor antagonist telmisartan were investigated in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial.
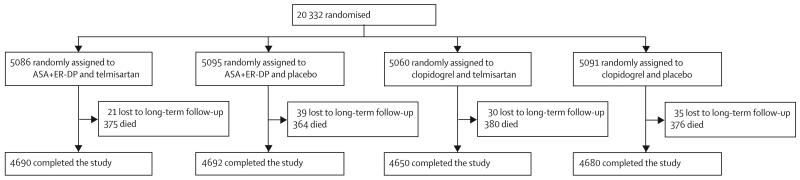
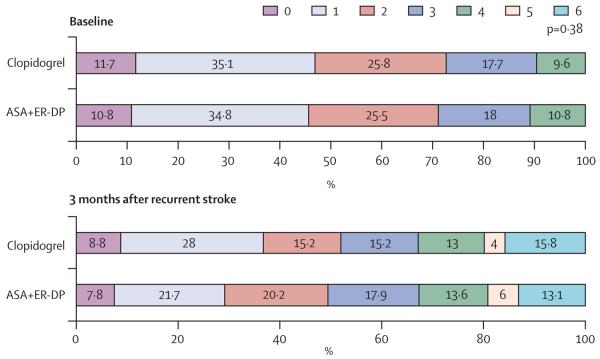
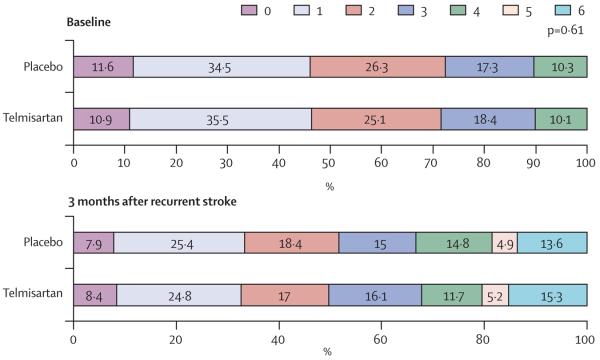
Methods: Patients who had had an ischaemic stroke were randomly assigned in a two by two factorial design to receive either 25 mg aspirin (ASA) and 200 mg extended-release dipyridamole (ER-DP) twice a day or 75 mg clopidogrel once a day, and either 80 mg telmisartan or placebo once per day. The predefined endpoints for this substudy were disability after a recurrent stroke, assessed with the modified Rankin scale (mRS) and Barthel index at 3 months, and cognitive function, assessed with the mini-mental state examination (MMSE) score at 4 weeks after randomisation and at the penultimate visit. Analysis was by intention to treat. The study was registered with ClinicalTrials.gov, number NCT00153062.
Findings: 20,332 patients (mean age 66 years) were randomised and followed-up for a median of 2.4 years. Recurrent strokes occurred in 916 (9%) patients randomly assigned to ASA with ER-DP and 898 (9%) patients randomly assigned to clopidogrel; 880 (9%) patients randomly assigned to telmisartan and 934 (9%) patients given placebo had recurrent strokes. mRS scores were not statistically different in patients with recurrent stroke who were treated with ASA and ER-DP versus clopidogrel (p=0.38), or with telmisartan versus placebo (p=0.61). There was no significant difference in the proportion of patients with recurrent stroke with a good outcome, as measured with the Barthel index, across all treatment groups. Additionally, there was no significant difference in the median MMSE scores, the percentage of patients with an MMSE score of 24 points or less, the percentage of patients with a drop in MMSE score of 3 points or more between 1 month and the penultimate visit, and the number of patients with dementia among the treatment groups. There were no significant differences in the proportion of patients with cognitive impairment or dementia among the treatment groups.
Interpretation: Disability due to recurrent stroke and cognitive decline in patients with ischaemic stroke were not different between the two antiplatelet regimens and were not affected by the preventive use of telmisartan.
Figures
Comment in
-
What do the results of the PRoFESS trial teach us?Lancet Neurol. 2008 Oct;7(10):860-2. doi: 10.1016/S1474-4422(08)70199-6. Epub 2008 Aug 29. Lancet Neurol. 2008. PMID: 18757237 No abstract available.
References
-
- De Keyser J, Uyttenboogaart M, Koch MW, et al. Neuroprotection in acute ischemic stroke. Acta Neurol Belg. 2005;105:144–48. - PubMed
-
- Schabitz WR, Fisher M. Perspectives on neuroprotective stroke therapy. Biochem Soc Trans. 2006;34:1271–76. - PubMed
-
- Hill MD. Stroke: the dashed hopes of neuroprotection. Lancet Neurol. 2007;6:2–3. - PubMed
-
- Zheng Z, Schwab S, Grau A, Berger C. Neuroprotection by early and delayed treatment of acute stroke with high dose aspirin. Brain. 2007;1186:275–80. - PubMed
-
- Gomes I. Aspirin: a neuroprotective agent at high doses? Natl Med J India. 1998;11:14–17. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
