

Lifetime risk of symptomatic knee osteoarthritis
- PMID: 18759314
- PMCID: PMC4516049
- DOI: 10.1002/art.24021
Lifetime risk of symptomatic knee osteoarthritis
Abstract
Objective: To estimate the lifetime risk of symptomatic knee osteoarthritis (OA), overall and stratified by sex, race, education, history of knee injury, and body mass index (BMI).
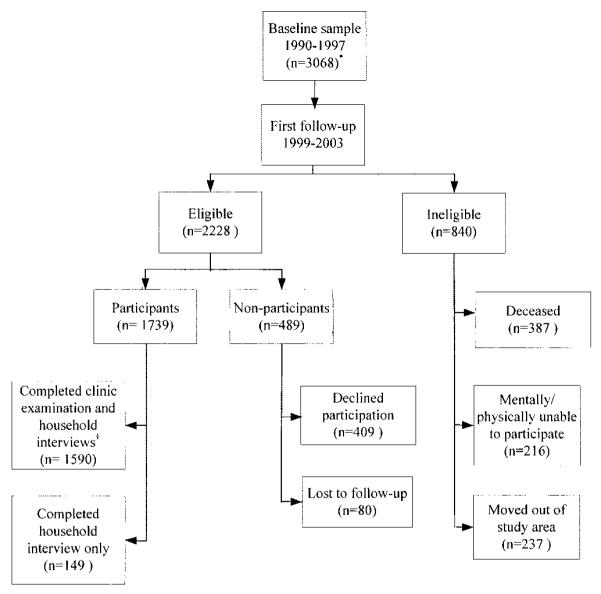
Methods: The lifetime risk of symptomatic OA in at least 1 knee was estimated from logistic regression models with generalized estimating equations among 3,068 participants of the Johnston County Osteoarthritis Project, a longitudinal study of black and white women and men age >or=45 years living in rural North Carolina. Radiographic, sociodemographic, and symptomatic knee data measured at baseline (1990-1997) and first followup (1999-2003) were analyzed.
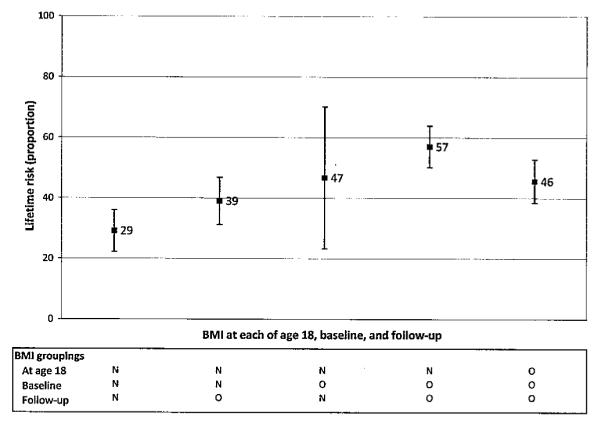
Results: The lifetime risk of symptomatic knee OA was 44.7% (95% confidence interval [95% CI] 40.0-49.3%). Cohort members with history of a knee injury had a lifetime risk of 56.8% (95% CI 48.4-65.2%). Lifetime risk rose with increasing BMI, with a risk of 2 in 3 among those who were obese.
Conclusion: Nearly half of the adults in Johnston County will develop symptomatic knee OA by age 85 years, with lifetime risk highest among obese persons. These current high risks in Johnston County may suggest similar risks in the general US population, especially given the increase in 2 major risk factors for knee OA, aging, and obesity. This underscores the immediate need for greater use of clinical and public health interventions, especially those that address weight loss and self-management, to reduce the impact of having knee OA.
Figures
References
-
- Centers for Disease Control and Prevention Prevalence of disabilities and associated health conditions among adults: United States, 1999. MMWR Morb Mortal Wkly Rep. 2001;50:120–5. - PubMed
-
- Kremers H, Gabriel S. Epidemiology of the rheumatic diseases: Kelley’s textbook of rheumatology. 7th ed Elsevier Saunders; Philadelphia: 2005. pp. 407–25.
-
- Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis Rheum. 1995;38:1134–41. - PubMed
-
- Agency for Healthcare Research and Quality National and regional statistics in the national inpatient sample, 2004. 2006 URL: http://www.hcup-us.ahrq.gov/nisoverview.jsp.
-
- Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991–94. J Rheumatol. 2006;33:2271–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
