

Reduction in rates of methicillin-resistant Staphylococcus aureus infection after introduction of quarterly linezolid-vancomycin cycling in a surgical intensive care unit
- PMID: 18759679
- PMCID: PMC2996816
- DOI: 10.1089/sur.2007.024
Reduction in rates of methicillin-resistant Staphylococcus aureus infection after introduction of quarterly linezolid-vancomycin cycling in a surgical intensive care unit
Abstract
Background: The burden of infection with antibiotic-resistant gram-positive cocci, including methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE), continues to increase, leading to substantial morbidity and high mortality rates, particularly in intensive care units (ICUs). Creative interventions may be required to reverse or stabilize this trend.
Methods: The efficacy of empiric cycling of antibiotics active against gram-positive organisms was tested in a before-after intervention in a single surgical ICU. Four years of baseline data were compared with two years of data compiled after the implementation of a strategy where the empiric antibiotic of choice for the treatment of gram-positive infections (linezolid or vancomycin) was changed every three months. Whatever the initial choice of drug, if possible, the antibiotic was de-escalated after final culture results were obtained. The rates of all gram-positive infections were analyzed, with a particular focus on MRSA and VRE. Concurrently, similar outcomes were followed for patients treated on the same services but outside the ICU, where cycling was not practiced.
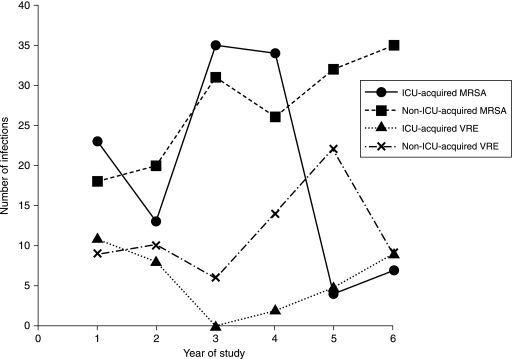
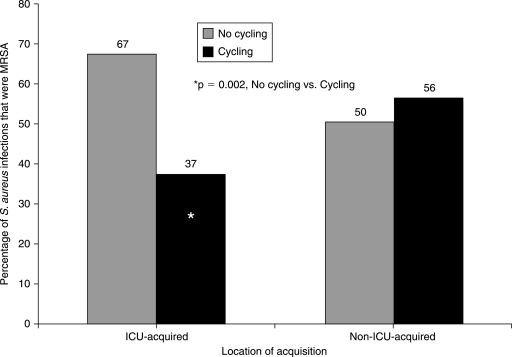
Results: During the four years prior to cycling, 543 infections with gram-positive organisms were acquired in the ICU (45.3/1,000 patient-days), including 105 caused by MRSA (8.8/1,000 patient days) and 21 by VRE (1.8/1,000 patient-days). In the two years after implementation of cycling, 169 gram-positive infections were documented (28.1/1,000 patient-days; p < 0.0001 vs. non-cycling period), including 11 caused by MRSA (1.8/1,000 patient-days; p < 0.0001 vs. non-cycling period). The percentage of S. aureus infections caused by MRSA declined from 67% to 36%. The rate of infection with VRE was unchanged. Outside the ICU, the yearly numbers of infections with both MRSA and VRE increased over time.
Conclusion: Quarterly cycling of linezolid and vancomycin in the ICU is a promising method to reduce infections with MRSA.
Figures
References
-
- Knaus WA. Draper EA. Wagner DP. Zimmerman JE. APACHE II: A severity of disease classification system. Crit Care Med. 1985;13:818–829. - PubMed
-
- Garner JS. Jarvis WR. Emori TG, et al. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16:128–140. - PubMed
-
- Gruson D. Hilbert G. Vargas F, et al. Rotation and restricted use of antibiotics in a medical intensive care unit: Impact on the incidence of ventilator-associated pneumonia caused by antibiotic-resistant gram-negative bacteria. Am J Respir Crit Care Med. 2000;162(3 Pt 1):837–843. - PubMed
-
- Raymond DP. Pelletier SJ. Crabtree TD, et al. Impact of a rotating empiric antibiotic schedule on infectious mortality in an intensive care unit. Crit Care Med. 2001;29:1101–1108. - PubMed
-
- Gruson D. Hilbert G. Vargas F, et al. Strategy of antibiotic rotation: Long-term effect on incidence and susceptibilities of gram-negative bacilli responsible for ventilator-associated pneumonia. Crit Care Med. 2003;31:1908–1914. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
