

Tirofiban preserves platelet loss during continuous renal replacement therapy in a randomised prospective open-blinded pilot study
- PMID: 18759963
- PMCID: PMC2575600
- DOI: 10.1186/cc6998
Tirofiban preserves platelet loss during continuous renal replacement therapy in a randomised prospective open-blinded pilot study
Abstract
Introduction: Approximately one third of all patients with cardiogenic shock suffer from acute kidney injury. Percutaneous coronary intervention, intra-aortic balloon pump, and continuous renal replacement therapy (CRRT) require effective antiplatelet therapy and anticoagulation, resulting in a high risk for platelet loss and bleeding events. The reversible platelet glycoprotein IIb/IIIa receptor inhibitor tirofiban was investigated to preserve platelet number and activation in a prospective open-blinded endpoint evaluation study.
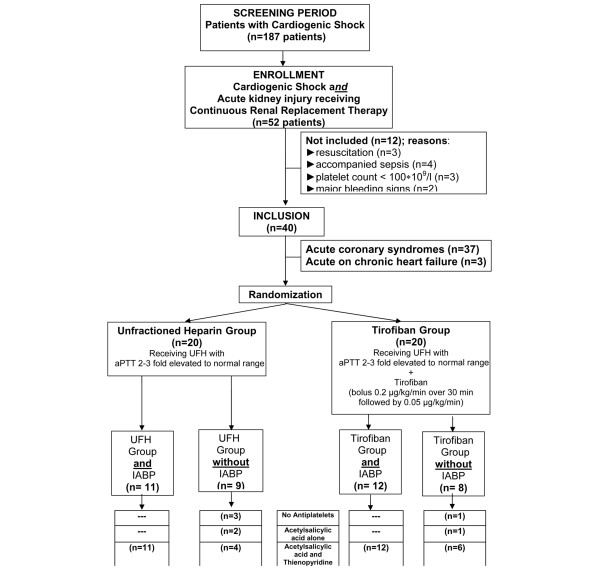
Methods: Forty patients with cardiogenic shock and acute kidney injury requiring CRRT were randomly assigned to two groups receiving unfractioned heparin (UFH) (n = 20) or a combined anticoagulation with UFH and tirofiban (n = 20). The primary endpoint was platelet loss during CRRT. Secondary endpoints were urea reduction, haemofilter life span, bleeding events, and necessity for platelet transfusions.
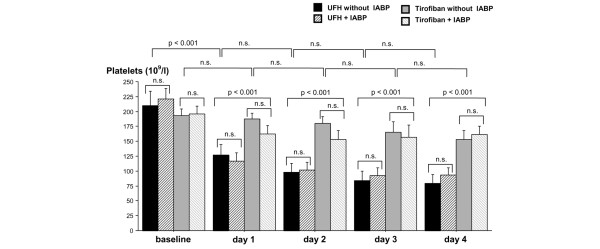
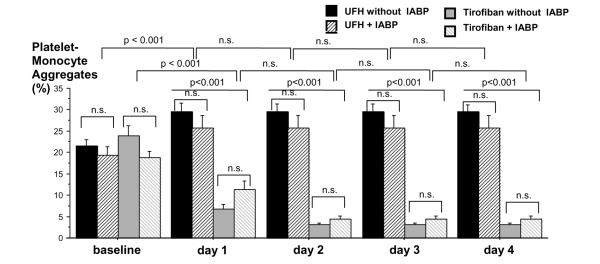
Results: In UFH-treated patients, the percentage of platelet-monocyte aggregates significantly increased (P < 0.001) and consecutively platelet cell count significantly decreased (P < 0.001). In contrast, combined treatment with UFH and tirofiban significantly decreased platelet-monocyte aggregates and platelet numbers (P < 0.001).
Conclusions: This pilot study provides evidence that the use of tirofiban in addition to UFH prevents platelet loss and preserves platelet function in patients with cardiogenic shock and acute kidney injury requiring CRRT. The pathophysiological inhibition of platelet aggregation and platelet-monocyte interaction appears to be causally involved.
Figures

Comment in
-
Does tirofiban prevent platelet loss in patients after cardiogenic shock during continuous renal replacement therapy?Crit Care. 2008;12(6):193. doi: 10.1186/cc7083. Epub 2008 Nov 24. Crit Care. 2008. PMID: 19040776 Free PMC article.
References
-
- Hochmann JS, Sleeper LA, White HD, Dzavik V, Wong SC, Menon V, Webb JG, Steingart R, Picard MH, Menegus MA, Boland J, Sanborn T, Buller CE, Modur S, Forman R, Desvigne-Nickens P, Jacobs AK, Slater JN, LeJemtel TH, SHOCK Investigators Should we emergently revascularize occluded coronaries for cardiogenic shock: one-year survival following early revascularization for cardiogenic shock. JAMA. 2001;285:190–192. doi: 10.1001/jama.285.2.190. - DOI - PubMed
-
- Bold J, Menges T, Wollbrück M, Sonneborn S, Hempelmann G. Continuous hemofiltration and platelet function in critically ill patients. Crit Care Med. 1994;22:1155–1160. - PubMed
-
- Mulder J, Tan HK, Bellomo R, Silvester W. Platelet loss across hemofilter during continuous hemofiltration. Int J Artif Organs. 2003;26:906–912. - PubMed
-
- Notohamiprodjo M, Andrassy K, Bommer J, Ritz E. Dialysis membranes and coagulation system. Blood. 1986;4:130–141. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
