

Infant brain probability templates for MRI segmentation and normalization
- PMID: 18761410
- PMCID: PMC2610429
- DOI: 10.1016/j.neuroimage.2008.07.060
Infant brain probability templates for MRI segmentation and normalization
Abstract
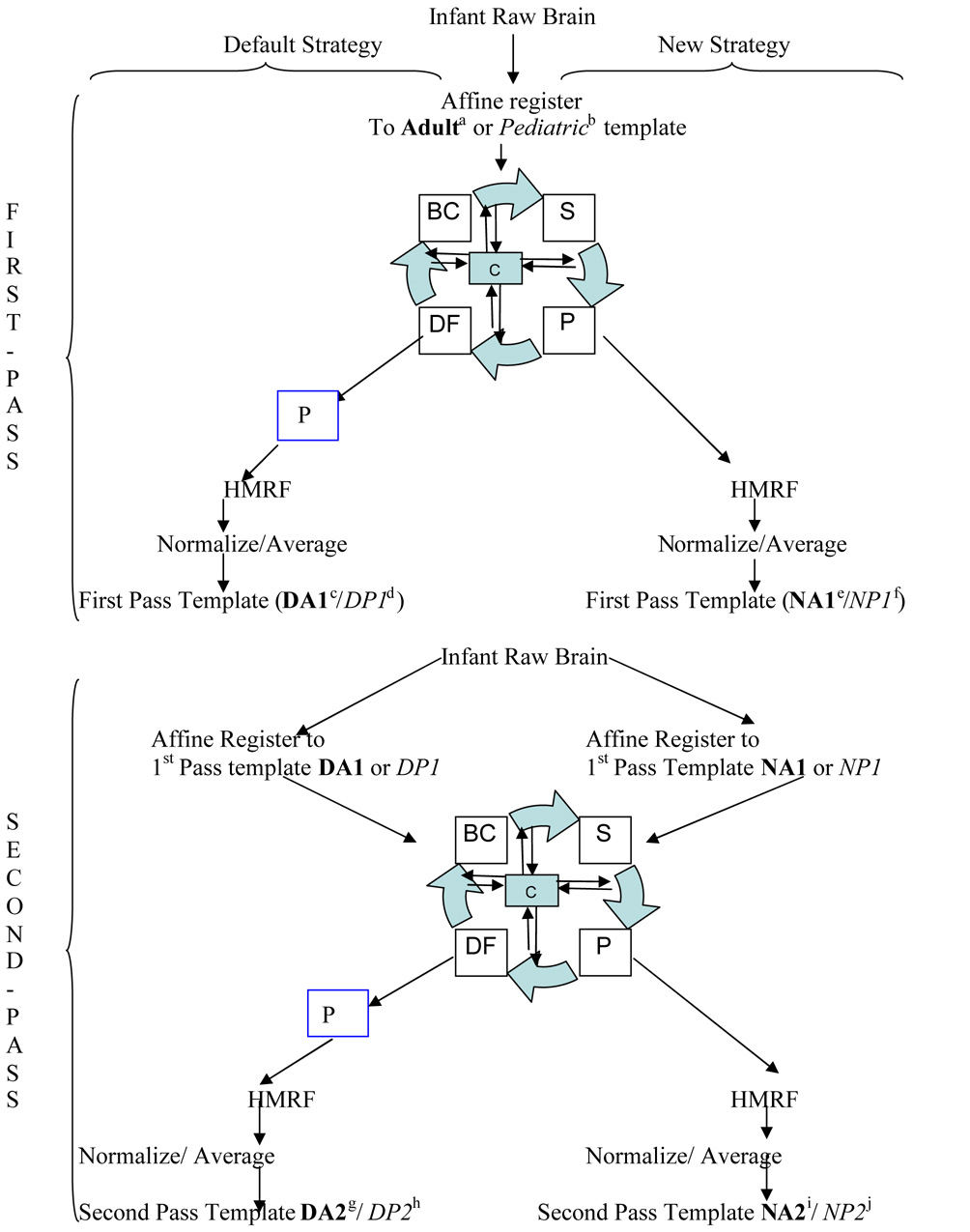
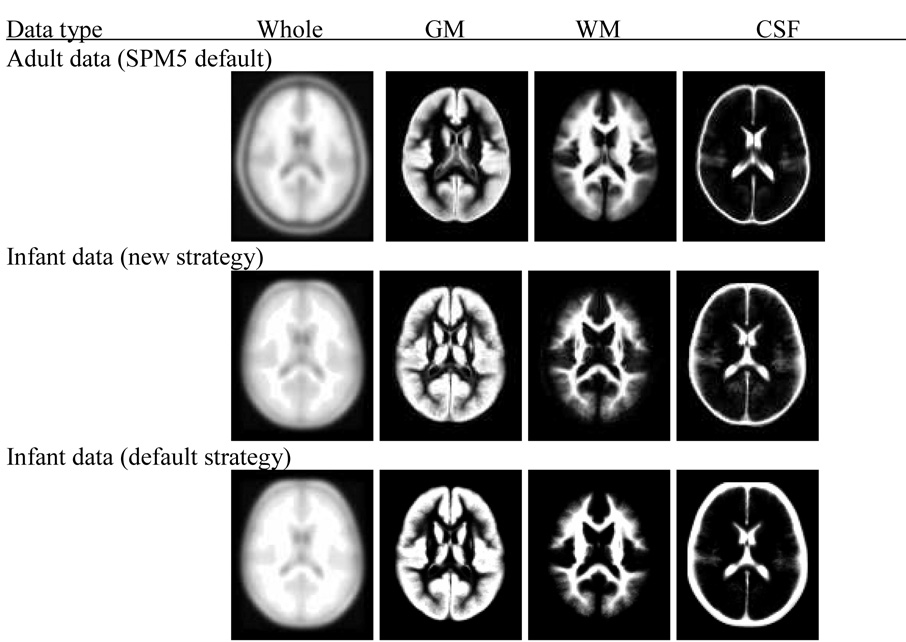
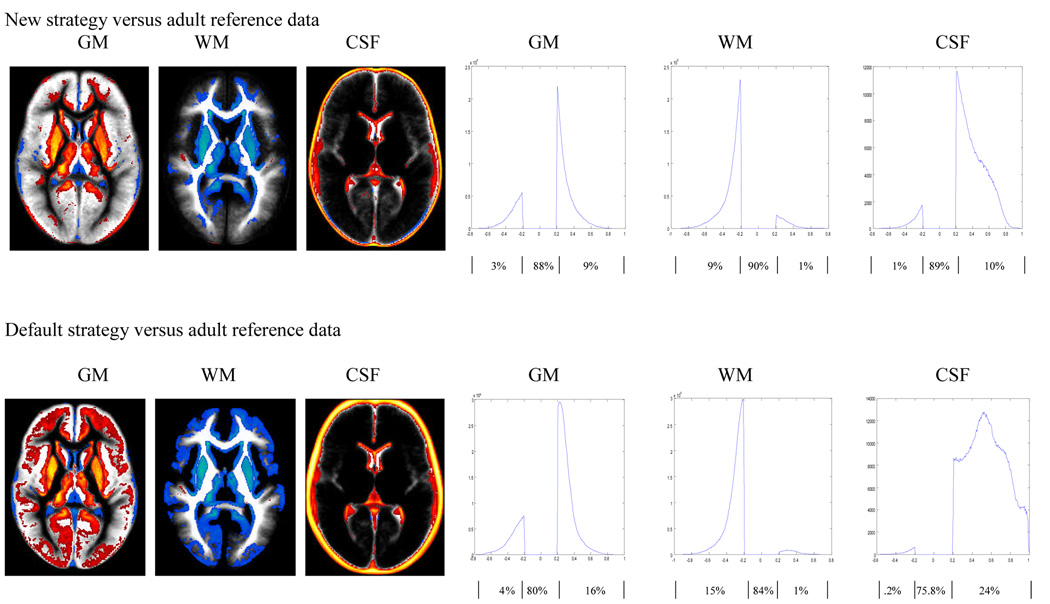
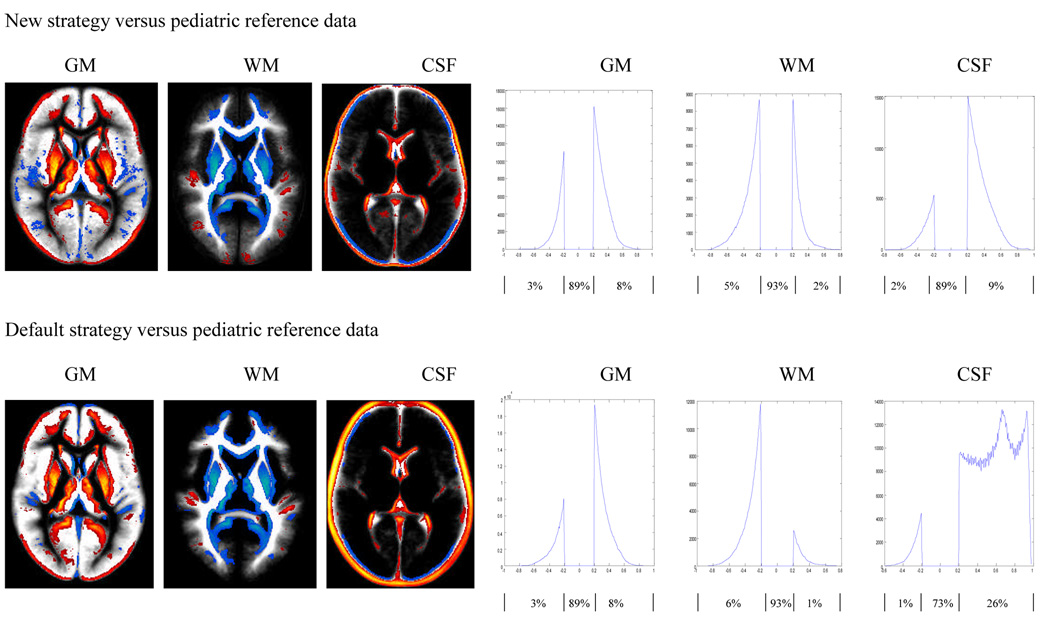
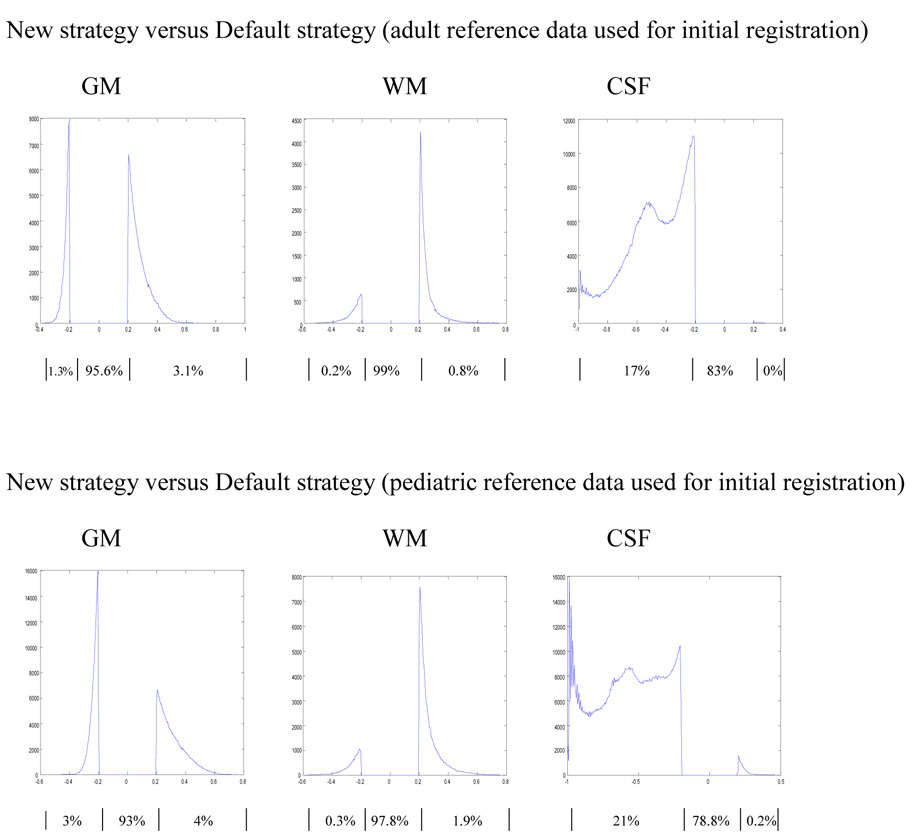
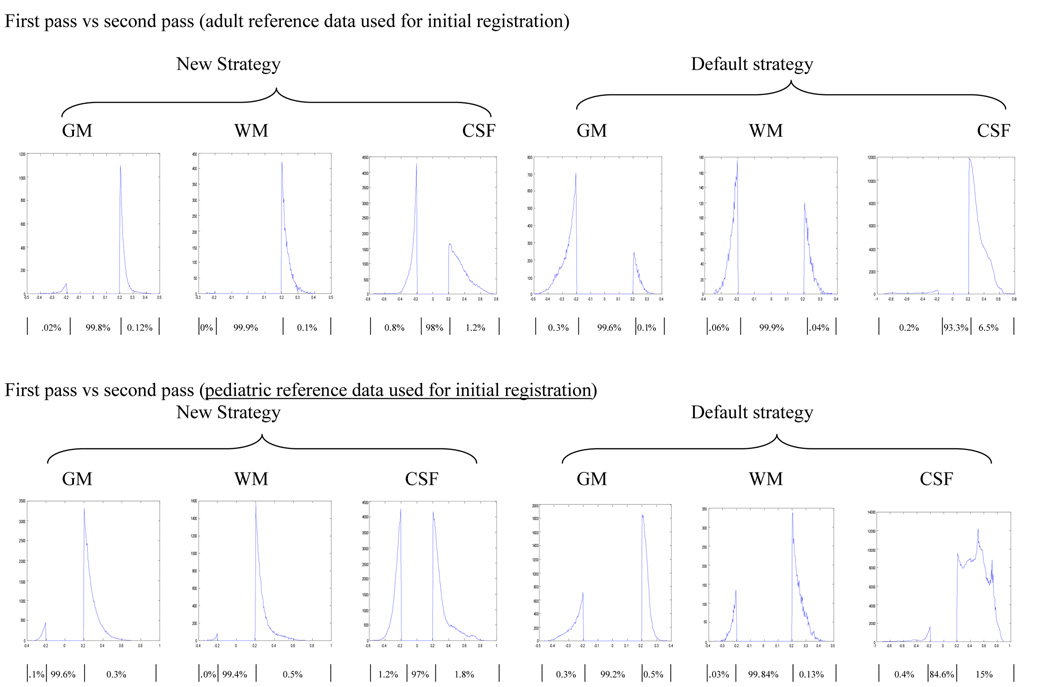
Spatial normalization and segmentation of infant brain MRI data based on adult or pediatric reference data may not be appropriate due to the developmental differences between the infant input data and the reference data. In this study we have constructed infant templates and a priori brain tissue probability maps based on the MR brain image data from 76 infants ranging in age from 9 to 15 months. We employed two processing strategies to construct the infant template and a priori data: one processed with and one without using a priori data in the segmentation step. Using the templates we constructed, comparisons between the adult templates and the new infant templates are presented. Tissue distribution differences are apparent between the infant and adult template, particularly in the gray matter (GM) maps. The infant a priori information classifies brain tissue as GM with higher probability than adult data, at the cost of white matter (WM), which presents with lower probability when compared to adult data. The differences are more pronounced in the frontal regions and in the cingulate gyrus. Similar differences are also observed when the infant data is compared to a pediatric (age 5 to 18) template. The two-pass segmentation approach taken here for infant T1W brain images has provided high quality tissue probability maps for GM, WM, and CSF, in infant brain images. These templates may be used as prior probability distributions for segmentation and normalization; a key to improving the accuracy of these procedures in special populations.
Figures
References
-
- Ashburner J, Friston KJ. Unified segmentation. NeuroImage. 2005;26:839–851. - PubMed
-
- Burgund ED, Kang HC, Kelly JE, Buckner RL, Snyder AZ, Petersen SE, Schlaggar BL. The feasibility of a common stereotactic space for children and adults in fMRI studies of development. NeuroImage. 2002;17:184–200. - PubMed
-
- Cuadra MB, Cammoun L, Butz T, Cuisenaire O, Thiran JP. Comparison and validation of tissue modelization and statistical classification methods in T1-weighted MR brain images. IEEE Trans Med Imaging. 2005;24:1548–1565. - PubMed
-
- Dehaene-Lambertz G, Dehaene S, Hertz-Pannier L. Functional neuroimaging of speech perception in infants. Science. 2002;298:2013–2015. - PubMed
-
- Evans AC, Collins DL, Mills SR, Brown ED, Kelly RL, Peters TM. 3D statistical neuroanatomical models from 305 MRI volumes. Proc. IEEE-Nucl Sci Symp Med Imaging Conf. 1993:1813–1817.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
