

Elevated temperature after hypoxic-ischemic encephalopathy: risk factor for adverse outcomes
- PMID: 18762517
- PMCID: PMC2782681
- DOI: 10.1542/peds.2007-1673
Elevated temperature after hypoxic-ischemic encephalopathy: risk factor for adverse outcomes
Abstract
Objective: The goal was to determine whether the risk of death or moderate/severe disability in term infants with hypoxic-ischemic encephalopathy increases with relatively high esophageal or skin temperature occurring between 6 and 78 hours after birth.
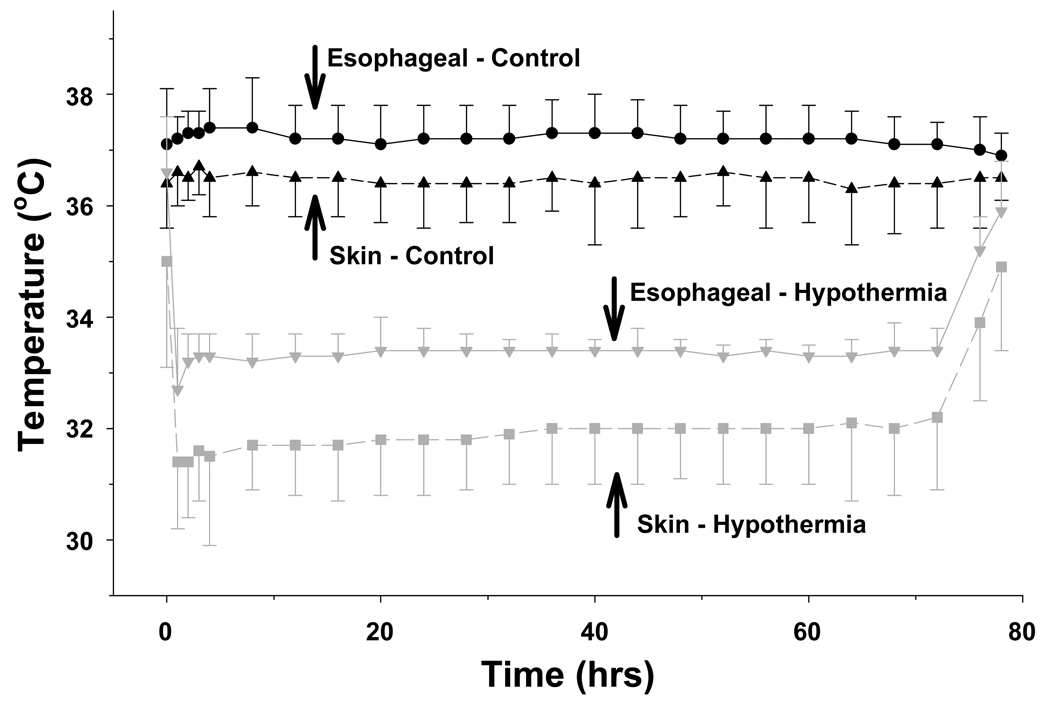
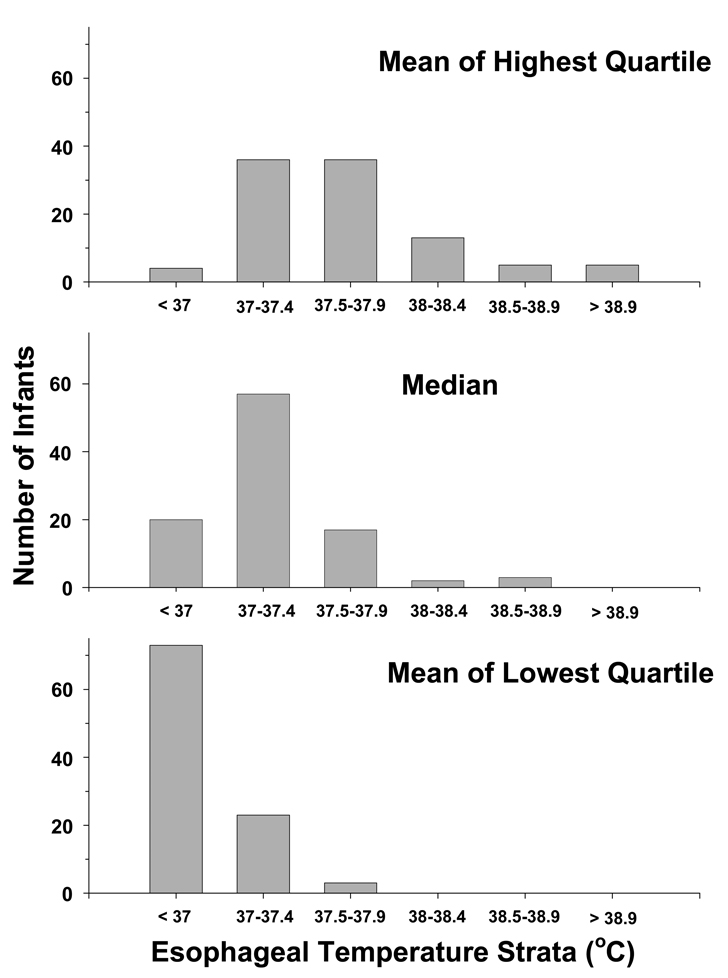
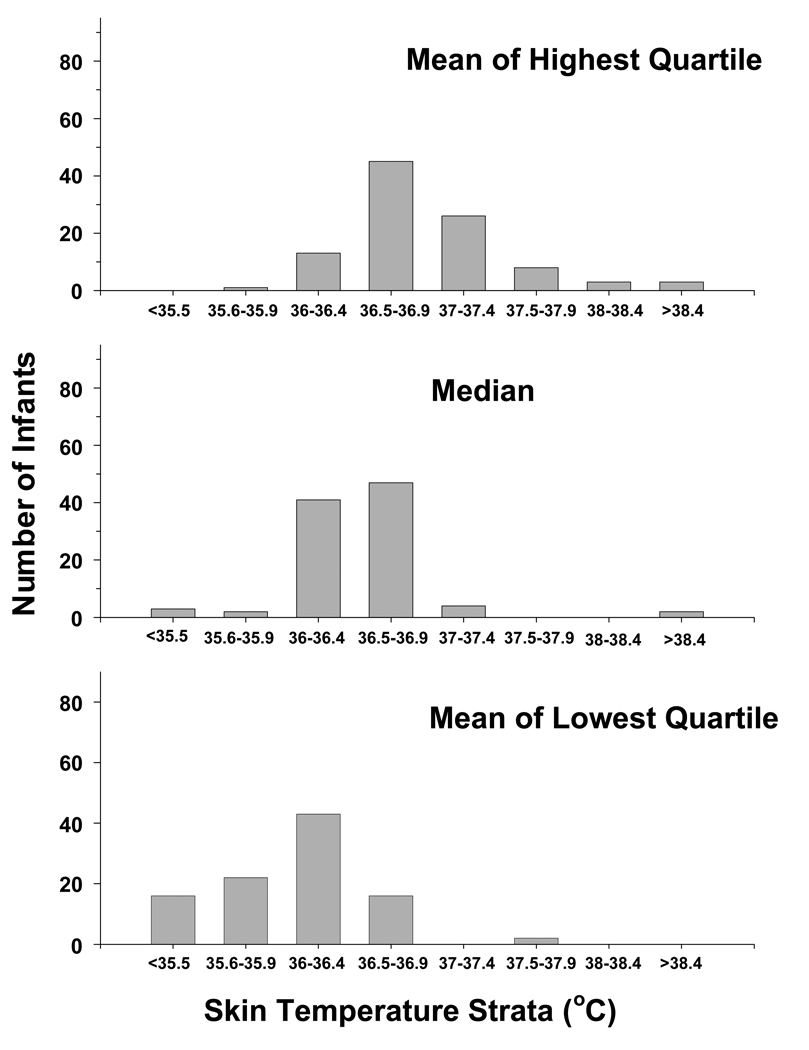
Methods: This was an observational secondary study within the National Institute of Child Health and Human Development Neonatal Research Network randomized trial comparing whole-body cooling and usual care (control) for term infants with hypoxic-ischemic encephalopathy. Esophageal and skin temperatures were recorded serially for 72 hours. Each infant's temperatures for each site were rank ordered. The high temperature was defined for each infant as the mean of all temperature measurements in the upper quartile. The low temperature was similarly defined as the mean of the lower quartile. Outcomes were related to temperatures in 3 logistic regression analyses for the high, median, and low temperatures at each temperature site for each group, with adjustment for the level of encephalopathy, gender, gestational age, and race.
Results: In control infants, the mean esophageal temperature was 37.2 +/- 0.7 degrees C over the 72-hour period, and 63%, 22%, and 8% of all temperatures were >37 degrees C, >37.5 degrees C, and >38 degrees C, respectively. The mean skin temperature was 36.5 +/- 0.8 degrees C, and 12%, 5%, and 2% of all temperatures were >37 degrees C, >37.5 degrees C, and >38 degrees C, respectively. The odds of death or disability were increased 3.6-4 fold for each 1 degrees C increase in the highest quartile of skin or esophageal temperatures. There were no associations between temperatures and outcomes in the cooling-treated group.
Conclusions: Relatively high temperatures during usual care after hypoxia-ischemia were associated with increased risk of adverse outcomes. The results may reflect underlying brain injury and/or adverse effects of temperature on outcomes.
Figures
References
-
- Paneth N. The causes of cerebral palsy. Recent evidence. Clin Invest Med. 1993;16(2):95–102. - PubMed
-
- Laptook AR, Corbett RJ. The effects of temperature on hypoxic-ischemic brain injury. Clin Perinatol. 2002;29(4):623–649. - PubMed
-
- Mishima K, Ikeda T, Yoshikawa T, Aoo N, Egashira N, Xia YX, et al. Effects of hypothermia and hyperthermia on attentional and spatial learning deficits following neonatal hypoxia-ischemic insult in rats. Behav Brain Res. 2004;151(1–2):209–217. - PubMed
-
- Yager JY, Armstrong EA, Jaharus C, Saucier DM, Wirrell EC. Preventing hyperthermia decreases brain damage following neonatal hypoxic-ischemic seizures. Brain Res. 2004;1011(1):48–57. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD27851/HD/NICHD NIH HHS/United States
- M01 RR 00125/RR/NCRR NIH HHS/United States
- M01RR 00039/RR/NCRR NIH HHS/United States
- M01 RR 00750/RR/NCRR NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD40689/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD 21373/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- U10 HD34216/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- U10 HD36790/HD/NICHD NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- M01 RR 08084/RR/NCRR NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- U10 HD40521/HD/NICHD NIH HHS/United States
- U10 HD27880/HD/NICHD NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- U10 HD27904/HD/NICHD NIH HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- U10 HD40498/HD/NICHD NIH HHS/United States
- U10 HD27871/HD/NICHD NIH HHS/United States
- M01 RR000044/RR/NCRR NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD27856/HD/NICHD NIH HHS/United States
- U10 HD40461/HD/NICHD NIH HHS/United States
- U10 HD27853/HD/NICHD NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- 5 M01 RR00044/RR/NCRR NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- M01 RR 00070/RR/NCRR NIH HHS/United States
- M01 RR 0039-43/RR/NCRR NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
- U10 HD21385/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
