

Lumbar discectomy outcomes vary by herniation level in the Spine Patient Outcomes Research Trial
- PMID: 18762639
- PMCID: PMC2657310
- DOI: 10.2106/JBJS.G.00913
Lumbar discectomy outcomes vary by herniation level in the Spine Patient Outcomes Research Trial
Abstract
Background: The Spine Patient Outcomes Research Trial showed an overall advantage for operative compared with nonoperative treatment of lumbar disc herniations. Because a recent randomized trial showed no benefit for operative treatment of a disc at the lumbosacral junction (L5-S1), we reviewed subgroups within the Spine Patient Outcomes Research Trial to assess the effect of herniation level on outcomes of operative and nonoperative care.
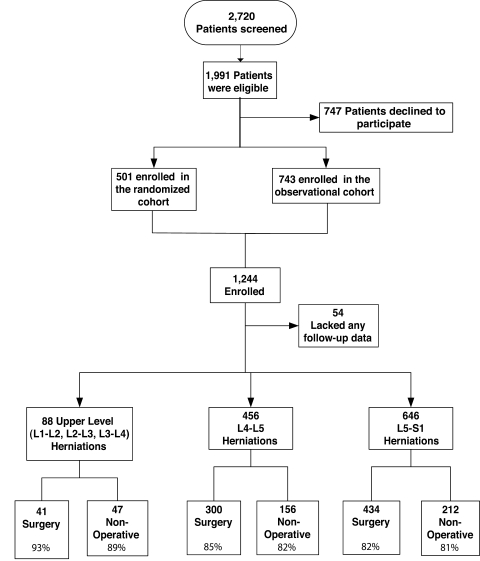
Methods: The combined randomized and observation cohorts of the Spine Patient Outcomes Research Trial were analyzed by actual treatment received stratified by level of disc herniation. Overall, 646 L5-S1 herniations, 456 L4-L5 herniations, and eighty-eight upper lumbar (L2-L3 or L3-L4) herniations were evaluated. Primary outcome measures were the Short Form-36 bodily pain and physical functioning scales and the modified Oswestry Disability Index assessed at six weeks, three months, six months, one year, and two years. Treatment effects (the improvement in the operative group minus the improvement in the nonoperative group) were estimated with use of longitudinal regression models, adjusting for important covariates.
Results: At two years, patients with upper lumbar herniations (L2-L3 or L3-L4) showed a significantly greater treatment effect from surgery than did patients with L5-S1 herniations for all outcome measures: 24.6 and 7.1, respectively, for bodily pain (p = 0.002); 23.4 and 9.9 for Short Form-36 physical functioning (p = 0.014); and -19 and -10.3 for Oswestry Disability Index (p = 0.033). There was a trend toward greater treatment effect for surgery at L4-L5 compared with L5-S1, but this was significant only for the Short Form-36 physical functioning subscale (p = 0.006). Differences in treatment effects between the upper lumbar levels and L4-L5 were significant for Short Form-36 bodily pain only (p = 0.018).
Conclusions: The advantage of operative compared with nonoperative treatment varied by herniation level, with the smallest treatment effects at L5-S1, intermediate effects at L4-L5, and the largest effects at L2-L3 and L3-L4. This difference in effect was mainly a result of less improvement in patients with upper lumbar herniations after nonoperative treatment.
Figures


References
-
- Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine Lumbar Spine Study. Spine. 2005;30:927-35. - PubMed
-
- Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation: a randomized controlled trial with 2 years of follow-up. Spine. 2006;31:2409-14. - PubMed
-
- Weber H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine. 1983;8:131-40. - PubMed
-
- Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson AN, Herkowitz H, Fischgrund J, Cammisa FP, Albert T, Deyo RA. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA. 2006;296:2451-9. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
