

Differentiation of malignant and benign proximal bile duct strictures: the diagnostic dilemma
- PMID: 18763286
- PMCID: PMC2742931
- DOI: 10.3748/wjg.14.5032
Differentiation of malignant and benign proximal bile duct strictures: the diagnostic dilemma
Abstract
Aim: To identify the criteria for the differentiation of hilar cholangiocarcinoma (HCCA) from benign strictures.
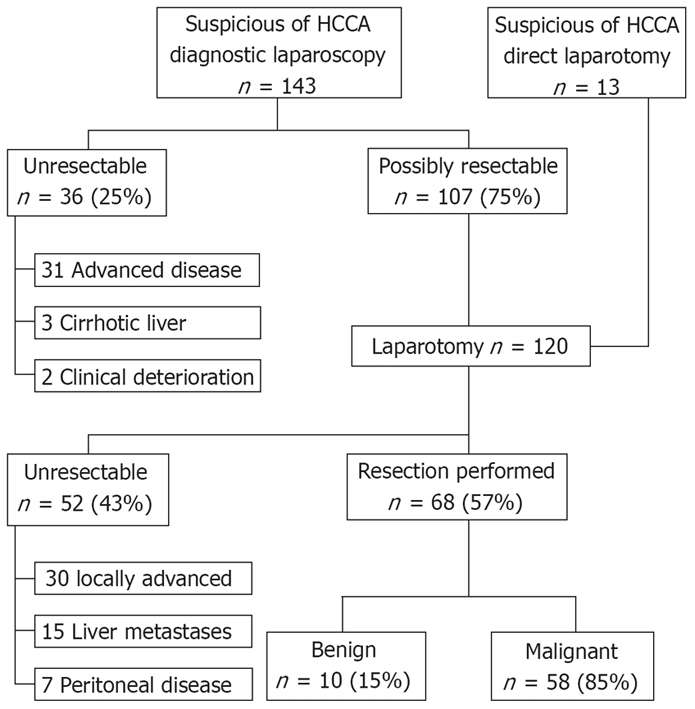
Methods: A total of 68 patients underwent resection of lesions suspicious for HCCA between 1998 and 2006. The results of laboratory investigations, imaging studies and brush cytology were collected. These findings were analyzed to obtain the final diagnosis.
Results: Histological examination of the resected specimens confirmed HCCA in 58 patients (85%, group I) whereas 10 patients (15%, group II) were diagnosed to have benign strictures. The most common presenting symptom was obstructive jaundice in 77% patients (79% group I vs 60% group II, P = 0.23). Laboratory findings showed greater elevation of transaminase levels in group I compared to group II. The various imaging modalities showed vascular involvement exclusively in the malignant group (36%, P < 0.05). Brush cytology was positive for malignant cells in only 50% patients in group I whereas none in group II showed malignant cells.
Conclusion: Despite improvements in imaging techniques, 10 patients (15%) with a presumptive diagnosis of HCCA were ultimately found to have benign strictures. Except for vascular involvement which was associated significantly with malignancy, there were no conclusive features of malignancy on regular imaging modalities. This uncertainty should be taken into account when patients with a suspicious lesion at the liver hilum are considered for resection.
Figures
References
-
- Witzigmann H, Berr F, Ringel U, Caca K, Uhlmann D, Schoppmeyer K, Tannapfel A, Wittekind C, Mossner J, Hauss J, et al. Surgical and palliative management and outcome in 184 patients with hilar cholangiocarcinoma: palliative photodynamic therapy plus stenting is comparable to r1/r2 resection. Ann Surg. 2006;244:230–239. - PMC - PubMed
-
- Dinant S, Gerhards MF, Rauws EA, Busch OR, Gouma DJ, van Gulik TM. Improved outcome of resection of hilar cholangiocarcinoma (Klatskin tumor) Ann Surg Oncol. 2006;13:872–880. - PubMed
-
- Looser C, Stain SC, Baer HU, Triller J, Blumgart LH. Staging of hilar cholangiocarcinoma by ultrasound and duplex sonography: a comparison with angiography and operative findings. Br J Radiol. 1992;65:871–877. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
