

Adaptive servoventilation (ASV) in patients with sleep disordered breathing associated with chronic opioid medications for non-malignant pain
- PMID: 18763421
- PMCID: PMC2542501
Adaptive servoventilation (ASV) in patients with sleep disordered breathing associated with chronic opioid medications for non-malignant pain
Abstract
Background: Adaptive servoventilation (ASV) can be effective therapy for specific types of central apnea such as Cheyne-Stokes respiration (CSR). Patients treated chronically with opioids develop central apneas and ataxic breathing patterns (Biot's respiration), but therapy with CPAP is usually unsuccessful. There are no published studies of ASV in patients with sleep apnea complicated by chronic opioid therapy.
Methods: Retrospective analysis of 22 consecutive patients referred for evaluation and treatment of sleep apnea who had been using opioid medications for at least 6 months, had an apnea-hypopnea index (AHI) > or = 20/h, and had been tested with ASV. Baseline polysomnography was compared with CPAP and ASV.
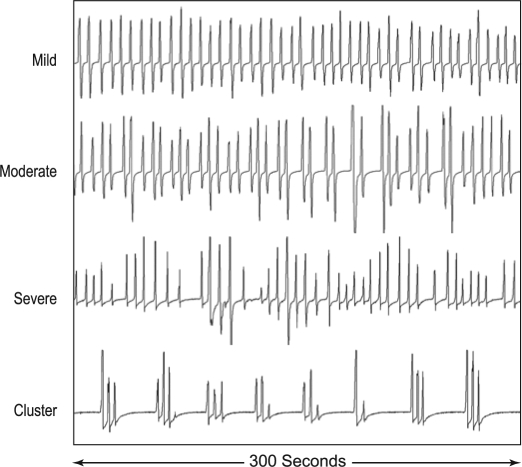
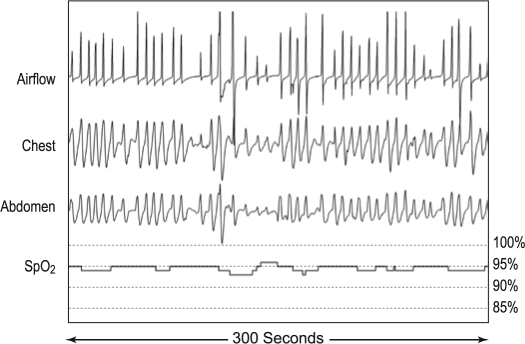
Outcome variables: AHI, central apnea index (CAI), obstructive apnea index (OAI), hypopnea index (HI), desaturation index, mean SpO2, lowest SpO2, time SpO2 < 90%, and degree of Biot's respiration.
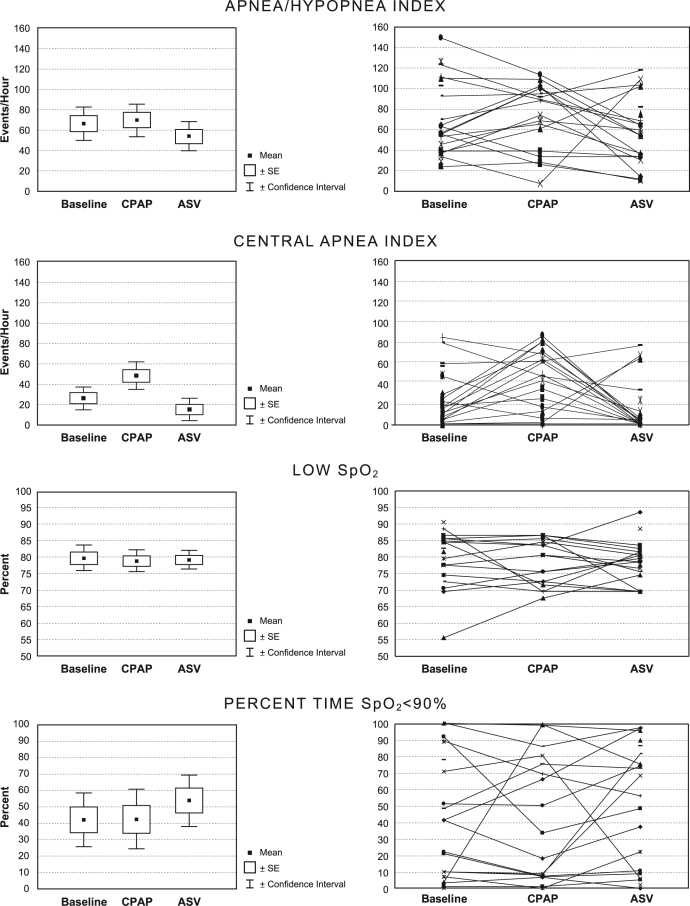
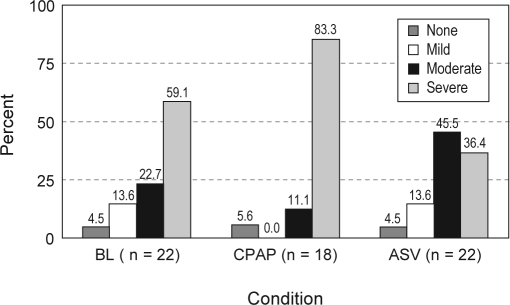
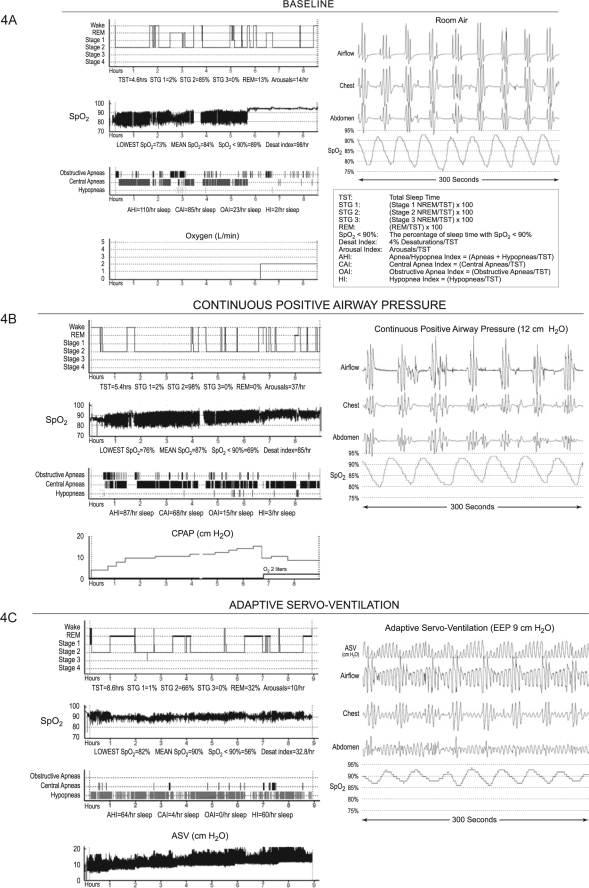
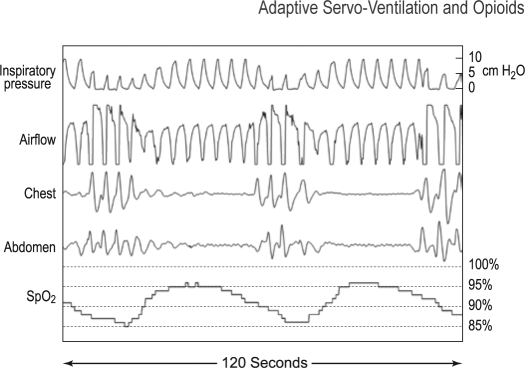
Results: Mean (SD) AHI measured 66.6/h (37.3) at baseline, 70.1/h (32.6) on CPAP, and 54.2/h (33.0) on ASV. With ASV, the mean OAI was significantly decreased to 2.4/h (p < 0.0001), and the mean HI increased significantly to 35.7/h (p < 0.0001). The decrease of CAI from 26.4/h to 15.6/h was not significant (p = 0.127). Biot's breathing persisted, and oxygenation parameters were unimproved with ASV.
Conclusions: Due to residual respiratory events and hypoxemia, ASV was considered insufficient therapy in these patients. Persistence of obstructive events could be due to suboptimal pressure settings (end expiratory and/or maximal inspiratory). Residual central events could be related to fundamental differences in the pathophysiology of CSR compared to opioid induced breathing disturbances.
Figures
Comment in
-
The quest for stability in an unstable world: adaptive servoventilation in opioid induced complex sleep apnea syndrome.J Clin Sleep Med. 2008 Aug 15;4(4):321-3. J Clin Sleep Med. 2008. PMID: 18763422 Free PMC article. No abstract available.
References
-
- Teschler H, Döhring J, Wang Y, et al. Adaptive pressure support servo-ventilation. A novel treatment for Cheyne-Stokes respiration in heart failure. Am J Respir Crit Care Med. 2001;164:614–19. - PubMed
-
- Pepperell JCT, Maskell NA, Jones DR, et al. A randomized controlled trial of adaptive ventilation for Cheyne-Stokes breathing in heart failure. Am J Respir Crit Care Med. 2003;168:1109–14. - PubMed
-
- Allam JS, Olson EJ, Gay PC, et al. Efficacy of adaptive servoventilation in treatment of complex and central sleep apnea syndromes. Chest. 2007;132:1839–46. - PubMed
-
- Morgenthaler TI, Gay PC, Gordon N, et al. Adaptive servoventilation versus noninvasive positive pressure ventilation for central, mixed and complex sleep apnea syndromes. Sleep. 2007;30:468–75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials