

Persistence of obstructive sleep apnea after surgical weight loss
- PMID: 18763424
- PMCID: PMC2542489
Persistence of obstructive sleep apnea after surgical weight loss
Abstract
Study objectives: Weight loss may reduce the severity of obstructive sleep apnea (OSA), but persistence of OSA following surgical weight loss has not been defined. We sought to clarify the impact of bariatric surgery on OSA. We hypothesized that, despite substantial weight loss and reductions in the apnea-hypopnea index (AHI), many will have persistent disease.
Methods: Consecutive patients referred for preoperative sleep evaluation underwent polysomnography before and 1 year following bariatric surgery. We compared the effects of weight loss on body mass, OSA, and continuous positive airway pressure requirements. We defined OSA severity using the AHI (normal < 5 events per hour, mild 5 to 14 events per hour, moderate 15 to 29 events per hour, and severe 30 or more events per hour). We identified predictors of OSA severity following weight loss and assessed compliance with therapy.
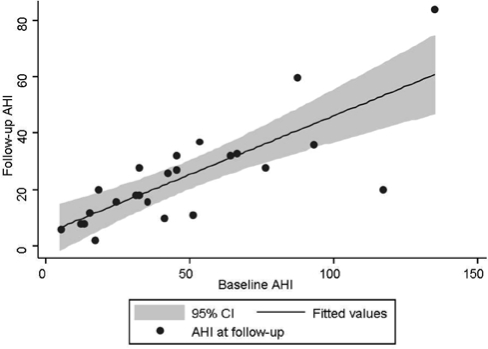
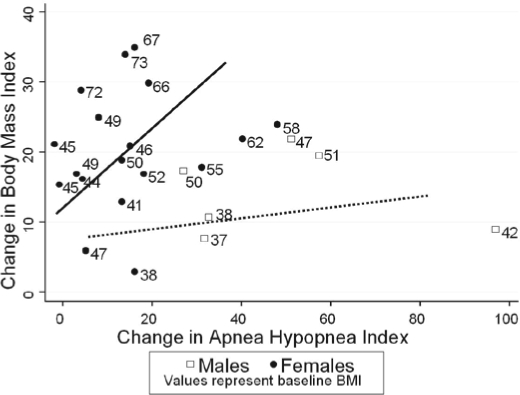
Results: Twenty-four patients (aged 47.9 +/- 9.3 years; 75% women) were enrolled. At baseline, all subjects had OSA, the majority of which was severe. Weight loss reduced body mass index from 51.0 +/- 10.4 kg/m2 to 32.1 +/- 5.5 kg/m2 (p < 0.001) and the AHI from 47.9 +/- 33.8 to 24.5 +/- 18.1 events per hour (p < 0.001). At follow-up, only 1 patient (4%) experienced resolution of OSA. The majority (71%) had moderate or severe disease. The most important predictor of the follow-up AHI was the baseline AHI (R2 = 0.603). All patients with residual OSA required continuous positive airway pressure to ablate apneic events, but the required pressures decreased from 11.5 +/- 3.6 cm H2O to 8.4 +/- 2.1 cm H20 (p = 0.001). Only 6 patients were compliant with continuous positive airway pressure therapy at the follow-up visit.
Conclusions: Surgical weight loss reduces the AHI, but many patients have residual OSA one year after bariatric surgery.
Figures
Comment in
-
Morbid obesity and sleep apnea. Is weight loss the answer?J Clin Sleep Med. 2008 Aug 15;4(4):339-40. J Clin Sleep Med. 2008. PMID: 18763425 Free PMC article. No abstract available.
References
-
- Health Implications of Obesity. NIH Consensus Development Conference Statement. Ann Intern Med. 1985;103:1073–7. - PubMed
-
- Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113:898–918. - PubMed
-
- Calle EE, Thun MJ, Petrelli JM, et al. Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med. 1999;341:1097–105. - PubMed
-
- Drenick EJ, Bale GS, Seltzer F, et al. Excessive mortality and causes of death in morbidly obese men. JAMA. 1980;243:443–5. - PubMed
-
- Garfinkel L. Overweight and cancer. Ann Intern Med. 1985;103:1034–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical