

Case Reports
doi: 10.1159/000151677.
Epub 2008 Sep 2.
Magnetocardiography-guided management of an unusual case of isoimmune complete atrioventricular block complicated by ventricular tachycardia
Affiliations
- PMID: 18765944
- PMCID: PMC2814147
- DOI: 10.1159/000151677
Item in Clipboard
Case Reports
Magnetocardiography-guided management of an unusual case of isoimmune complete atrioventricular block complicated by ventricular tachycardia
Fetal Diagn Ther.
2008.
Abstract
A fetus who was diagnosed at 25 weeks of gestation with isoimmune AV block presented at 34 weeks with a precipitous fall in ventricular rate and periods of tachycardia. Magnetocardiography revealed the tachycardia to be ventricular. After delivery, nonsustained ventricular tachycardia continued. The baby then successfully paced, and at higher ventricular rates the tachycardia resolved. Five years later the child has normal ventricular function and is doing well.
Copyright 2008 S. Karger AG, Basel.
Figures

Fetal heart rate patterns of acceleration. Each individual black line is an R-R interval. The graph shows the heart rate over 5 min. A At 28 weeks, the tracing shows good variability over a wide ventricular rate range. B At 34 weeks, not only has the ventricular rate dropped precipitously, but there is no variability whatsoever in the ventricular rate range. The tall lines represent ventricular ectopy.
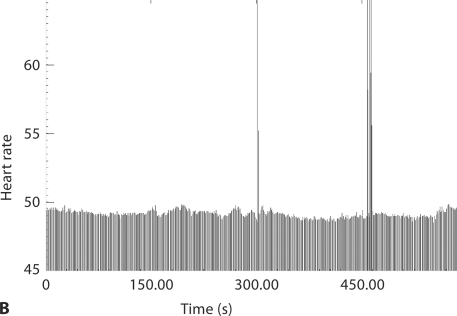
Fetal heart rate patterns of acceleration. Each individual black line is an R-R interval. The graph shows the heart rate over 5 min. A At 28 weeks, the tracing shows good variability over a wide ventricular rate range. B At 34 weeks, not only has the ventricular rate dropped precipitously, but there is no variability whatsoever in the ventricular rate range. The tall lines represent ventricular ectopy.

Fetal magnetocardiograph at 34 weeks gestation from 3 of the 37 channels. The lower channel displays the maternal QRS (arrows). Note that the QRS complexes of ventricular origin are distinct from intrinsic narrow QRS complexes of the fetus' escape rhythm. The ventricular arrhythmia appears to be nearly monomorphic, suggesting a single focus. These QRS complexes are not likely to reflect aberrancy of intermittent AV conducted beats because the ventricular rate is faster than the atrial rate. Between episodes of ventricular arrhythmia, AV dissociation can be appreciated with apparent resetting of the intrinsic ventricular escape rhythm. Bottom tracing is maternal in origin.

Postnatal 12-lead electrocardiogram in the newborn with congenital complete AV block and ventricular arrhythmias documented by fMCG. Baseline artifact is seen. Atrial rate is 166 bpm, ventricular rate is 45 bpm, QT interval is 485 ms, and QTc is 442 ms.
References
-
- Wakai RT, Leuthold AC, Cripe L, Martin CB. Assessment of fetal rhythm in complete congenital heart block by magnetocardiography. PACE. 2000;23:1047–1050. - PubMed
-
- Wakai TR, Leuthold AC, Martin CB. Atrial and ventricular fetal heart rate patterns in isolated congenital complete heart block detected by magnetocardiography. Am J Obstet Gynecol. 1998;179:258–260. - PubMed
-
- Mendez T, Achenbach S, Beinder E, Hofbeck M, Klinghammer L, Singer H, Moshage W, Daniel WG. Usefulness of magnetocardiography for the investigation of fetal arrhythmias. Am J Cardiol. 2001;88:334–836. - PubMed
-
- Wakai RT, Strasburger JF, Li Z, Deal BJ, Gotteiner NL. Magnetocardiographic rhythm patterns at initiation and termination of fetal supraventricular tachycardia. Circulation. 2003;107:307–312. - PubMed
-
- Cuneo BF, Ovadia M, Strasburger JF, et al. Prenatal diagnosis and in utero treatment of torsades de pointes associated with congenital long QT syndrome. Am J Cardiol. 2003;91:1395–1398. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
