

Treatment of localised resectable neuroblastoma. Results of the LNESG1 study by the SIOP Europe Neuroblastoma Group
- PMID: 18766186
- PMCID: PMC2567095
- DOI: 10.1038/sj.bjc.6604640
Treatment of localised resectable neuroblastoma. Results of the LNESG1 study by the SIOP Europe Neuroblastoma Group
Abstract
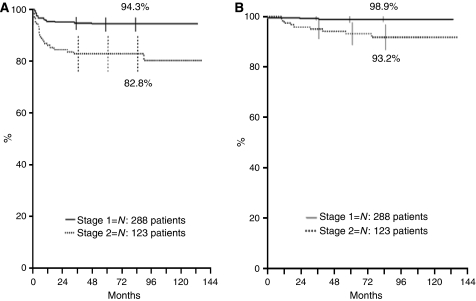
Main objective of this study was to confirm that surgery alone is an effective and safe treatment for localised resectable neuroblastoma except stage 2 with amplified MYCN gene (MYCNA). Of 427 eligible stages 1-2 patients, 411 had normal MYCN and 16 had MYCNA. Of the 288 stage 1 patients with normal MYCN, 1 died of complications and 16 relapsed, 2 of whom died; 5-year relapse-free survival (RFS) and overall survival (OS) rates were 94.3% (95% confidence interval (CI): 91.6-97) and 98.9% (95% CI: 97.7-100), respectively. Of the 123 stage 2 patients with normal MYCN, 1 died of sepsis and 22 relapsed, 8 of whom died (RFS 82.8%, 95% CI: 76.2-89.5; OS 93.2%, 95% CI: 88.7-97.8). In stage 2, OS and RFS were worse for patients with elevated LDH and unfavourable histopathology. Of 16 children with MYCNA, 7 were stage 1 (5 relapses and 4 deaths) and 9 were stage 2 (3 relapses and 2 deaths) patients. In conclusion, surgery alone yielded excellent OS for both stage 1 and 2 neuroblastoma without MYCNA, although stage 2 patients with unfavourable histopathology and elevated LDH suffered a high number of relapses. Both stage 1 and 2 patients with MYCNA were at greater risk of relapse.
Figures
Similar articles
-
Influence of image-defined risk factors on the outcome of patients with localised neuroblastoma. A report from the LNESG1 study of the European International Society of Paediatric Oncology Neuroblastoma Group.Pediatr Blood Cancer. 2015 Sep;62(9):1536-42. doi: 10.1002/pbc.25460. Epub 2015 Feb 8. Pediatr Blood Cancer. 2015. PMID: 25663103
-
MYCN oncogene amplification in neuroblastoma is associated with worse prognosis, except in stage 4s: the Italian experience with 295 children.J Clin Oncol. 1997 Jan;15(1):85-93. doi: 10.1200/JCO.1997.15.1.85. J Clin Oncol. 1997. PMID: 8996128
-
Localized resectable neuroblastoma: results of the second study of the Italian Cooperative Group for Neuroblastoma.J Clin Oncol. 1995 Apr;13(4):884-93. doi: 10.1200/JCO.1995.13.4.884. J Clin Oncol. 1995. PMID: 7707115 Clinical Trial.
-
Relationship between histopathological features, MYCN amplification, and prognosis: a UKCCSG study. United Kingdom Children Cancer Study Group.Med Pediatr Oncol. 2001 Jan;36(1):169-76. doi: 10.1002/1096-911X(20010101)36:1<169::AID-MPO1041>3.0.CO;2-U. Med Pediatr Oncol. 2001. PMID: 11464876 Review.
-
Prognostic significance of MYCN oncogene expression in childhood neuroblastoma.J Clin Oncol. 1998 Oct;16(10):3286-94. doi: 10.1200/JCO.1998.16.10.3286. J Clin Oncol. 1998. PMID: 9779703 Review.
Cited by
-
Segmental chromosomal aberrations as the poor prognostic factor in children over 18 months with stage 3 neuroblastoma without MYCN amplification.Front Oncol. 2023 Feb 14;13:1134772. doi: 10.3389/fonc.2023.1134772. eCollection 2023. Front Oncol. 2023. PMID: 36865795 Free PMC article.
-
Revisions to the International Neuroblastoma Response Criteria: A Consensus Statement From the National Cancer Institute Clinical Trials Planning Meeting.J Clin Oncol. 2017 Aug 1;35(22):2580-2587. doi: 10.1200/JCO.2016.72.0177. Epub 2017 May 4. J Clin Oncol. 2017. PMID: 28471719 Free PMC article. Review.
-
Advances in liquid biopsy in neuroblastoma.Fundam Res. 2022 Aug 17;2(6):903-917. doi: 10.1016/j.fmre.2022.08.005. eCollection 2022 Nov. Fundam Res. 2022. PMID: 38933377 Free PMC article. Review.
-
Integrated bulk and single-cell RNA sequencing reveals a cuproptosis-related LncRNA prognostic signature in neuroblastoma.BMC Cancer. 2025 Jul 1;25(1):1076. doi: 10.1186/s12885-025-14463-8. BMC Cancer. 2025. PMID: 40596995 Free PMC article.
-
Prognostic value of ferritin, neuron-specific enolase, lactate dehydrogenase, and urinary and plasmatic catecholamine metabolites in children with neuroblastoma.Onco Targets Ther. 2012;5:417-23. doi: 10.2147/OTT.S36366. Epub 2012 Nov 30. Onco Targets Ther. 2012. PMID: 23226699 Free PMC article.
References
-
- Alvarado CS, London WB, Look AT, Brodeur GM, Altmiller DH, Thorner PS, Joshi VV, Rowe ST, Nash MB, Smith EI, Castleberry RP, Cohn SL (2000) Natural history and biology of stage A neuroblastoma: a Pediatric Oncology Group Study. J Pediatr Hematol Oncol 22: 197–205 - PubMed
-
- Ambros IM, Benard J, Boavida M, Bown N, Caron H, Combaret V, Couturier J, Darnfors C, Delattre O, Freeman-Edward J, Gambini C, Gross N, Hattinger CM, Luegmayr A, Lunec J, Martinsson T, Mazzocco K, Navarro S, Noguera R, O’Neill S, Potschger U, Rumpler S, Speleman F, Tonini GP, Valent A, Van Roy N, Amann G, De Bernardi B, Kogner P, Ladenstein R, Michon J, Pearson AD, Ambros PF (2003) Quality assessment of genetic markers used for therapy stratification. J Clin Oncol 21: 2077–2084 - PubMed
-
- Bagatell R, Rumcheva P, London WB, Cohn SL, Look AT, Brodeur GM, Frantz C, Joshi V, Thorner P, Rao PV, Castleberry R, Bowman LC (2005) Outcomes of children with intermediate-risk neuroblastoma after treatment stratified by MYCN status and tumour cell ploidy. J Clin Oncol 23: 8819–8827 - PubMed
-
- Brodeur GM, Pritchard J, Berthold F, Carlsen NL, Castel V, Castelberry RP, De Bernardi B, Evans AE, Favrot M, Hedborg F (1993) Revisions of the international criteria for neuroblastoma diagnosis, staging, and response to treatment. J Clin Oncol 11: 1466–1477 - PubMed
-
- Caron HN, Pearson ADJ (2005) Neuroblastoma. In Cancer in Children, Voûte PA, Barrett A, Stevens MCG, Caron HN (eds), 5th edn, pp 337–352, Oxford University Press: Oxford
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
