

Prognostic importance of defibrillator shocks in patients with heart failure
- PMID: 18768944
- PMCID: PMC2922510
- DOI: 10.1056/NEJMoa071098
Prognostic importance of defibrillator shocks in patients with heart failure
Abstract
Background: Patients with heart failure who receive an implantable cardioverter-defibrillator (ICD) for primary prevention (i.e., prevention of a first life-threatening arrhythmic event) may later receive therapeutic shocks from the ICD. Information about long-term prognosis after ICD therapy in such patients is limited.
Methods: Of 829 patients with heart failure who were randomly assigned to ICD therapy, we implanted the ICD in 811. ICD shocks that followed the onset of ventricular tachycardia or ventricular fibrillation were considered to be appropriate. All other ICD shocks were considered to be inappropriate.
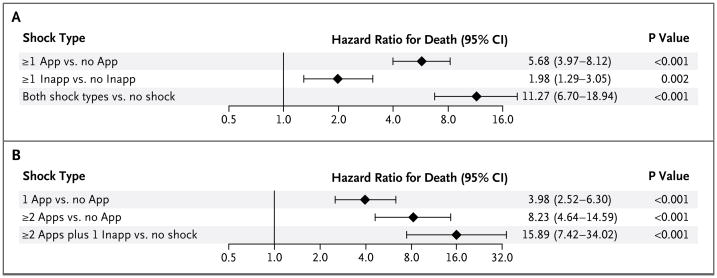
Results: Over a median follow-up period of 45.5 months, 269 patients (33.2%) received at least one ICD shock, with 128 patients receiving only appropriate shocks, 87 receiving only inappropriate shocks, and 54 receiving both types of shock. In a Cox proportional-hazards model adjusted for baseline prognostic factors, an appropriate ICD shock, as compared with no appropriate shock, was associated with a significant increase in the subsequent risk of death from all causes (hazard ratio, 5.68; 95% confidence interval [CI], 3.97 to 8.12; P<0.001). An inappropriate ICD shock, as compared with no inappropriate shock, was also associated with a significant increase in the risk of death (hazard ratio, 1.98; 95% CI, 1.29 to 3.05; P=0.002). For patients who survived longer than 24 hours after an appropriate ICD shock, the risk of death remained elevated (hazard ratio, 2.99; 95% CI, 2.04 to 4.37; P<0.001). The most common cause of death among patients who received any ICD shock was progressive heart failure.
Conclusions: Among patients with heart failure in whom an ICD is implanted for primary prevention, those who receive shocks for any arrhythmia have a substantially higher risk of death than similar patients who do not receive such shocks.
2008 Massachusetts Medical Society
Figures

Comment in
-
Life and death after ICD implantation.N Engl J Med. 2008 Sep 4;359(10):1058-9. doi: 10.1056/NEJMe0806103. N Engl J Med. 2008. PMID: 18768951 No abstract available.
References
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Fishbein DP. SCD-HeFT Investigators. Sudden Cardiac Death-Heart Failure Trial (SCD-HeFT) In: Woosley RL, Singh SN, editors. Arrhythmia treatment and therapy. New York: Marcel Dekker; 2000. pp. 323–42.
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardio-verter–defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. [Erratum, N Engl J Med 2005;352:2146.] - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;51:2085–105. - PubMed
-
- Moss AJ, Greenberg H, Case RB, et al. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation. 2004;110:3760–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical