

Has management of epidermoid tumors of the cerebellopontine angle improved? A surgical synopsis of the past and present
- PMID: 18769651
- PMCID: PMC2435477
- DOI: 10.1055/s-2007-991108
Has management of epidermoid tumors of the cerebellopontine angle improved? A surgical synopsis of the past and present
Abstract
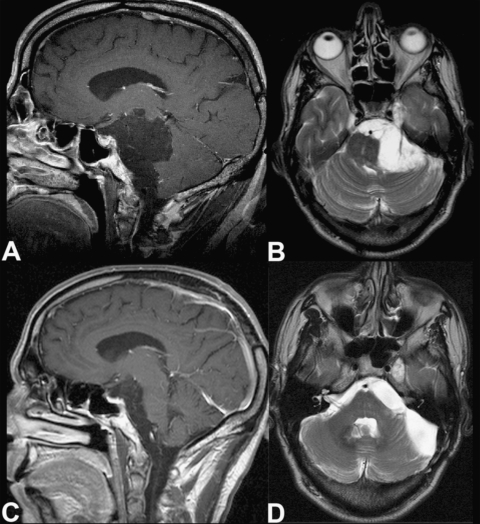
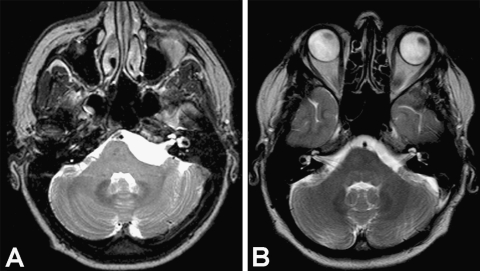
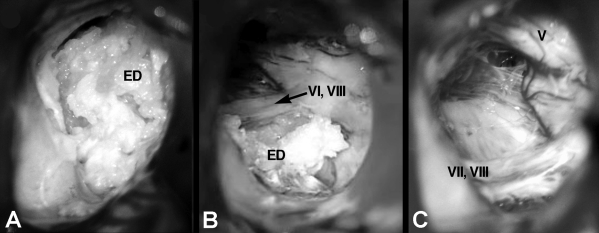
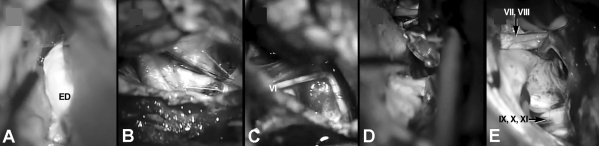
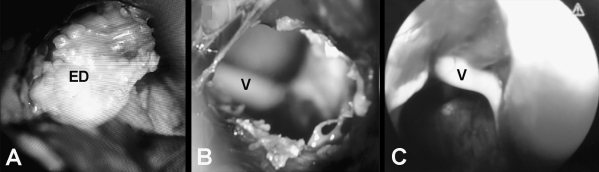
We compared the surgical outcomes of recent patients with cerebellopontine angle (CPA) epidermoids treated with advanced surgical tools with those of patients treated in earlier series. From November 2000 to June 2004, we treated 12 patients with epidermoid tumors. One patient had a strict CPA lesion. Tumors extended into the prepontine region in seven cases and supratentorially in two. In two cases the CPA was involved bilaterally. All patients but one underwent a lateral suboccipital approach in a semi-sitting position with microsurgical technique. Endoscopic assistance was used in cases with extensions beyond the CPA. In one case, a subtemporal route was used. The mean follow-up was 27 months (range, 8 to 50 months). There were no deaths. Total removal was achieved in 7 of the 10 patients with unilateral CPA epidermoids. Preoperative status improved in eight (80%) patients, particularly the function of cranial nerves (CNs) V and VII. Only two patients had permanent CN deficits. Complete excision with preservation of CN function should be the goals of management of epidermoids of the CPA. In some cases, these goals can be difficult to achieve, even with contemporary surgical equipment. Bilateral and extensive tumors should be removed in staged procedures. The function of CN V and CN VII may recover after decompression, but the outcome of symptoms related to CN VIII is less certain. The endoscope is a reliable tool for assessing the extension of epidermoids, but it cannot be used for tumor removal.
Keywords: Epidermoid; cerebellopontine angle; cranial nerve deficits; suboccipital; subtemporal.
Figures
References
-
- Caldarelli M, Massimi L, Kondageski C, Di Rocco C. Intracranial midline dermoid and epidermoid cysts in children. J Neurosurg. 2004;100:473–480. - PubMed
-
- Berger M S, Wilson C B. Epidermoid cysts of the posterior fossa. J Neurosurg. 1985;62:214–219. - PubMed
-
- Gagliardi F M, Vagnozzi R, Caruso R, Delfini R. Epidermoids of the cerebellopontine angle (cpa): usefulness of CT scan. Acta Neurochir (Wien) 1980;54:271–281. - PubMed
-
- Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinical course and surgical prognosis of 33 cases of intracranial epidermoid tumors. Neurosurgery. 1989;24:568–573. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
