

Validation of creatinine assays utilizing HPLC and IDMS traceable standards in sera of children
- PMID: 18769945
- PMCID: PMC2788619
- DOI: 10.1007/s00467-008-0957-0
Validation of creatinine assays utilizing HPLC and IDMS traceable standards in sera of children
Abstract
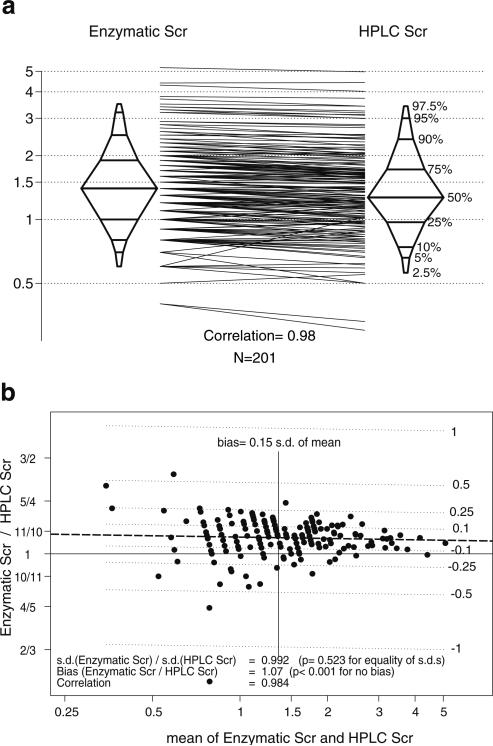
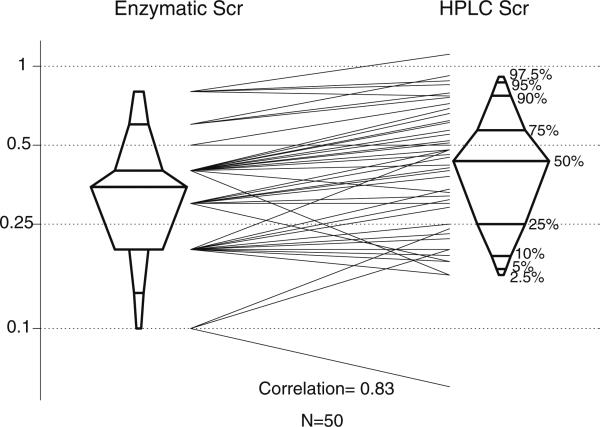
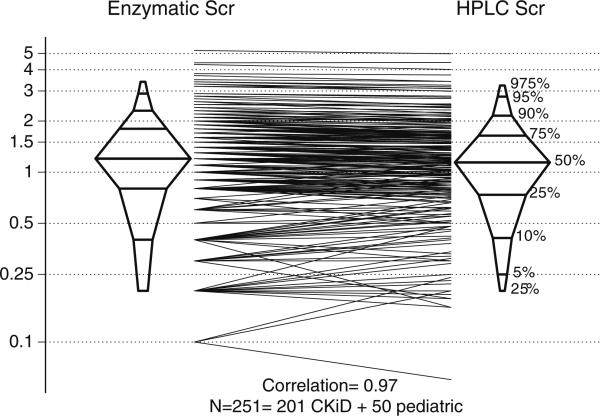
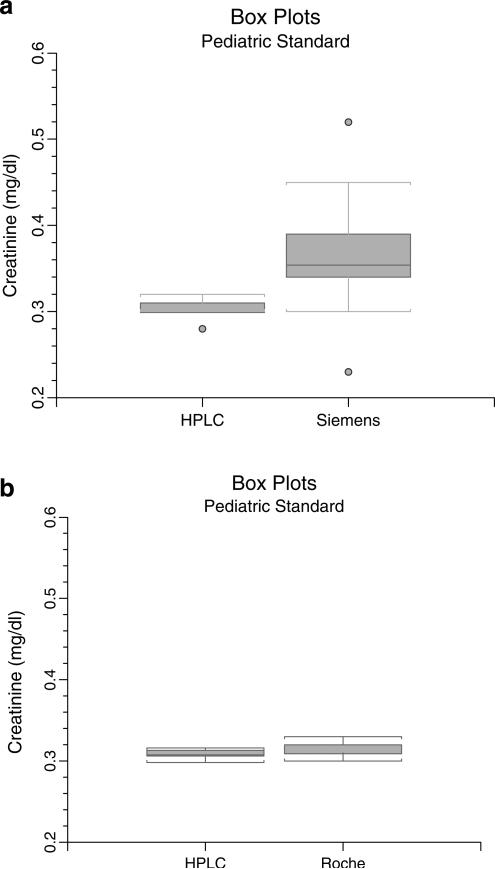
The purpose of this study was to validate serum creatinine (SCr) concentrations assayed in the Central Biochemistry Laboratory of the National Institutes of Health (NIH)-funded Chronic Kidney Disease in Children (CKiD) study utilizing an enzymatic assay (Siemens Advia 2400) against a method traceable to reference isotope dilution mass spectroscopy (IDMS) developed by the National Institute of Standards and Technology (NIST). High-performance liquid chromatography (HPLC) measured SCr after external validation utilizing IDMS-based standard reference materials. Sera from the first 201 subjects enrolled in CKiD were analyzed and compared for creatinine concentration by enzymatic and HPLC methods. Fifty "normal" pediatric sera were subsequently analyzed. Finally, a "pediatric" reference standard was prepared and examined for accuracy and precision. Enzymatic SCr concentrations (median 1.4 mg/dl) of CKiD subjects were well correlated with HPLC (r = 0.984) but were slightly higher (+7%; p < 0.001). Agreement was poorer at lower SCr (median 0.4 mg/dl) when using samples from normal children and the "pediatric" reference standard. However, the Roche enzymatic assay was comparable with HPLC in accuracy and precision. Referring physicians should be aware of the accuracy and reproducibility of their laboratory's SCr assay. Our enzymatic assay agreed well with HPLC in CKiD subjects with elevated SCr. We suggest that NIST develop a pediatric SCr standard reference material for use by assay manufacturers to improve accuracy and precision of assays at the low SCr levels observed in most pediatric patients.
Figures
References
-
- Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am. 1987;34:571–590. - PubMed
-
- Hogg RJ, Furth S, Lemley KV, Portman R, Schwartz GJ, Coresh J, Balk E, Lau J, Levin A, Kausz AT, Eknoyan G, Levey AS. National Kidney Foundation's kidney disease outcomes quality initiative clinical practice guidelines for chronic kidney disease in children and adolescents: evaluation, classification, and stratification. Pediatrics. 2003;111:1416–1421. - PubMed
-
- Myers GL, Miller WG, Coresh J, Fleming J, Greenberg N, Greene T, Hostetter T, Levey AS, Panteghini M, Welch M, Eckfeldt JH. Recommendations for improving serum creatinine measurement: a report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin Chem. 2006;52:5–18. - PubMed
-
- Levey AS, Bosch JP, Lewis JB, Greene T, Rogers NL, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999;130:461–470. - PubMed
-
- Schwartz GJ, Haycock GB, Chir B, Spitzer A. Plasma creatinine and urea concentration in children: normal values for age and sex. J Pediatr. 1976;88:828–830. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
