

Experimental model of warfarin-associated intracerebral hemorrhage
- PMID: 18772448
- PMCID: PMC3712841
- DOI: 10.1161/STROKEAHA.108.517482
Experimental model of warfarin-associated intracerebral hemorrhage
Abstract
Background and purpose: Future demographic changes predict an increase in the number of patients with atrial fibrillation. As long-term anticoagulation for the prevention of ischemic strokes becomes more prevalent, the burden of warfarin-associated intracerebral hemorrhage (W-ICH) is likely to grow. However, little is known about the clinical aspects and pathophysiologic mechanisms of W-ICH. This study describes the development of a mouse model of W-ICH in which hematoma growth and outcomes can be correlated with anticoagulation parameters.
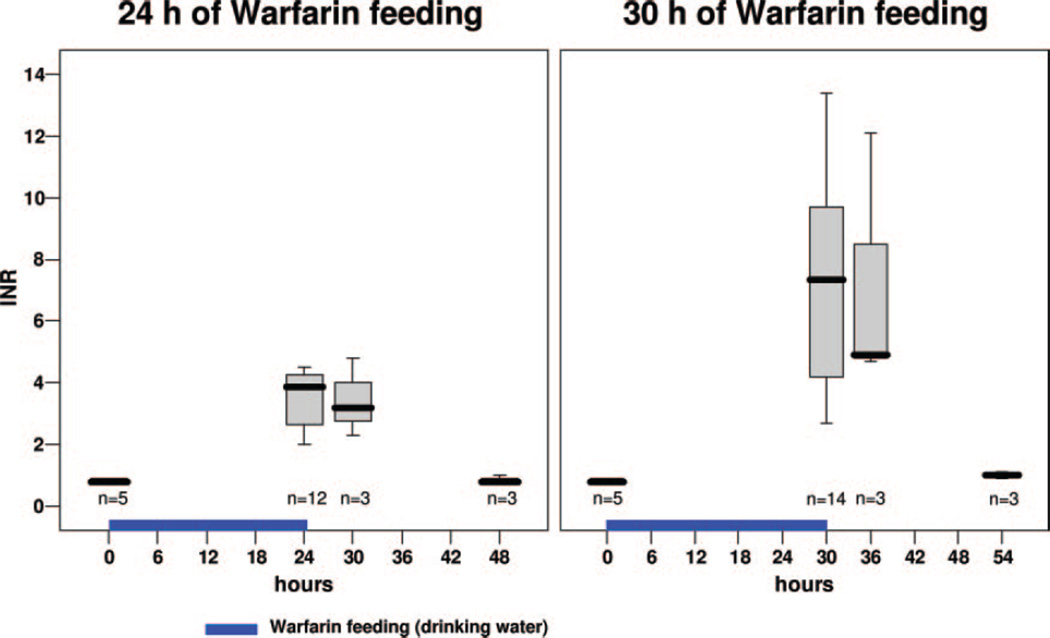
Methods: CD-1 mice were treated with warfarin (2 mg/kg per 24 hours) added to drinking water. ICH was induced by stereotactic injection of collagenase type VII (0.075 U) into the right striatum. Hemorrhagic blood volume was quantified by means of a photometric hemoglobin assay 2 and 24 hours after hemorrhage induction. Neurologic outcomes were assessed on a 5-point scale.
Results: The international normalized ratio in nonanticoagulated mice was 0.8+/-0.1. After 24 (W-24) and 30 (W-30) hours of warfarin pretreatment, international normalized ratio values increased to 3.5+/-0.9 and 7.2+/-3.4, respectively. Compared with nonanticoagulated mice, mean hemorrhagic blood volume determined 24 hours after hemorrhage induction was found to be 2.5-fold larger in W-24 mice (P=0.019) and 3.1-fold larger in W-30 mice (P<0.001, n=10 per group). Mortality at 24 hours after hemorrhage induction was 0% in nonanticoagulated mice, 10% in W-24 mice, and 30% in W-30 mice. Hematoma enlargement between 2 and 24 hours after hemorrhage induction was -1.4% for nonanticoagulated mice, 22.9% for W-24 mice, and 62.2% for W-30 mice.
Conclusions: This study characterizes the first experimental model of W-ICH. It may be helpful in gaining further insights into the pathophysiology of W-ICH and may be used for testing the efficacy of treatment strategies, such as hemostatic therapy, in this severe subtype of stroke.
Figures




References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Go AS. The epidemiology of atrial fibrillation in elderly persons: the tip of the iceberg. Am J Geriatr Cardiol. 2005;14:56–61. - PubMed
-
- Kucher N, Castellanos LR, Quiroz R, Koo S, Fanikos J, Goldhaber SZ. Time trends in warfarin-associated hemorrhage. Am J Cardiol. 2004;94:403–406. - PubMed
-
- Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions. Stroke. 2006;37:256–262. - PubMed
-
- Flaherty ML, Kissela B, Woo D, Kleindorfer D, Alwell K, Sekar P, Moomaw CJ, Haverbusch M, Broderick JP. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 2007;68:116–121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
