

Is preoperative histological diagnosis necessary before referral to major surgery for cholangiocarcinoma?
- PMID: 18773064
- PMCID: PMC2504385
- DOI: 10.1080/13651820802014585
Is preoperative histological diagnosis necessary before referral to major surgery for cholangiocarcinoma?
Abstract
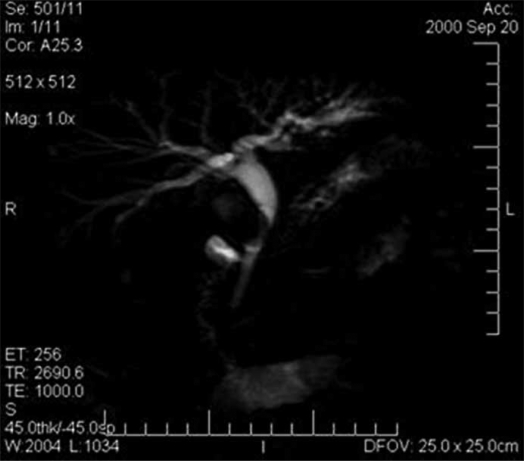
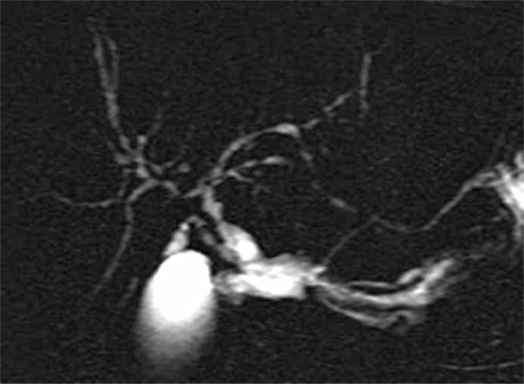
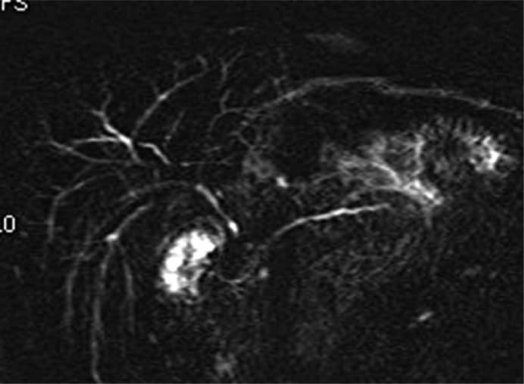
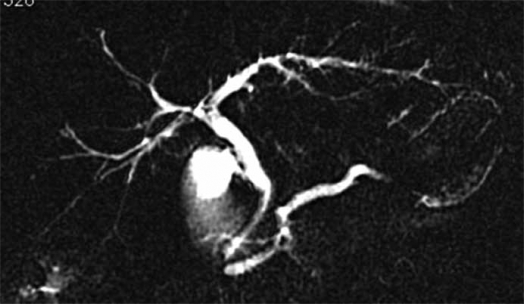
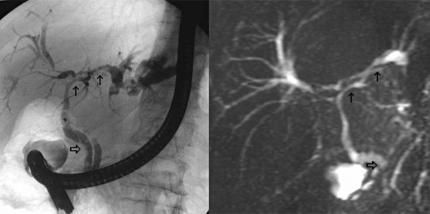
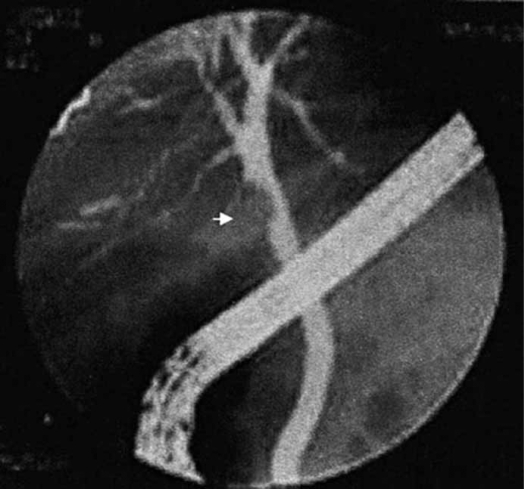
Major surgical resection is often the only curative treatment for cholangiocarcinoma. When imaging techniques fail to establish the accurate diagnosis, biopsy of the lesion is unavoidable. However, biopsy is not necessarily required for topography of the cholangiocarcinoma (intrahepatic or extrahepatic). 1) In extrahepatic cholangiocarcinoma (ECC), clinical features and radiological imaging relate to biliary obstruction. Provided that between 8% and 43% of bile duct strictures are not ECC, the lesions mimicking ECC that should be ruled out are gallbladder cancer, Mirizzi syndrome, primary sclerosing cholangitis (PSC), autoimmune pancreatitis and portal biliopathy. Systematic biopsy is usually difficult and has poor sensitivity, but a good knowledge of these mimicking ECC diseases, along with precise analysis of clinical and imaging semiology, may lead to a correct diagnosis without the need for biopsy. 2) Intrahepatic cholangiocarcinoma (ICC) developing in normal liver appears as a hypovascular tumour with fibrotic component and capsular retraction that can be confused with fibrous metastases such as breast and colorectal cancers. The lack of the primary site, a relatively large tumour size and ancillary findings such as bile duct dilatation may provide a clue to the diagnosis. If not, we advocate local resection with lymph node dissection, since ICC is the most likely diagnosis and surgery is the only curative treatment. In the event of adenocarcinoma from unknown primary, surgery is an effective treatment even if prognosis is poor.
Figures
Similar articles
-
Immunoglobulin G4-associated sclerosing cholangitis mimicking cholangiocarcinoma.Hong Kong Med J. 2010 Apr;16(2):149-52. Hong Kong Med J. 2010. PMID: 20354252
-
Clinical clues to suspicion of IgG4-associated sclerosing cholangitis disguised as primary sclerosing cholangitis or hilar cholangiocarcinoma.J Gastroenterol Hepatol. 2010 Dec;25(12):1831-7. doi: 10.1111/j.1440-1746.2010.06411.x. J Gastroenterol Hepatol. 2010. PMID: 21091993
-
IgG4-related sclerosing cholangitis in the absence of autoimmune pancreatitis mimicking extrahepatic cholangiocarcinoma.Scand J Gastroenterol. 2015 Apr;50(4):447-53. doi: 10.3109/00365521.2014.962603. Epub 2015 Jan 30. Scand J Gastroenterol. 2015. PMID: 25635498
-
Imaging Features of Primary Sclerosing Cholangitis: From Diagnosis to Liver Transplant Follow-up.Radiographics. 2019 Nov-Dec;39(7):1938-1964. doi: 10.1148/rg.2019180213. Epub 2019 Oct 18. Radiographics. 2019. PMID: 31626561 Review.
-
Adult bile duct strictures: role of MR imaging and MR cholangiopancreatography in characterization.Radiographics. 2014 May-Jun;34(3):565-86. doi: 10.1148/rg.343125211. Radiographics. 2014. PMID: 24819781 Review.
Cited by
-
Bile Duct Lithiasis Mimicking a Perihilar Cholangiocarcinoma-An Endless Dilemma: A Case Report.J Clin Med. 2023 Aug 3;12(15):5104. doi: 10.3390/jcm12155104. J Clin Med. 2023. PMID: 37568507 Free PMC article.
-
Fascioliasis simulating an intrahepatic cholangiocarcinoma-Case report with imaging and pathology correlation.Hepatobiliary Surg Nutr. 2015 Feb;4(1):E1-7. doi: 10.3978/j.issn.2304-3881.2014.09.15. Hepatobiliary Surg Nutr. 2015. PMID: 25713810 Free PMC article.
-
Outcome of surgical resection in Klatskin tumors.World J Gastrointest Oncol. 2013 Jul 15;5(7):147-58. doi: 10.4251/wjgo.v5.i7.147. World J Gastrointest Oncol. 2013. PMID: 23919109 Free PMC article.
-
Approach to Solid Liver Masses in the Cirrhotic Patient.Gastroenterology Res. 2009 Oct;2(5):259-267. doi: 10.4021/gr2009.10.1314. Epub 2009 Sep 20. Gastroenterology Res. 2009. PMID: 27956969 Free PMC article. Review.
-
A pancreatic mass and extreme elevation of CA 19-9: a benign masquerade of cholangiocarcinoma.J Surg Case Rep. 2022 Feb 16;2022(2):rjac018. doi: 10.1093/jscr/rjac018. eCollection 2022 Feb. J Surg Case Rep. 2022. PMID: 35186252 Free PMC article.
References
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–25. - PubMed
-
- Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet. 2005;366:1303–14. - PubMed
-
- Are C, Gonen M, D'Angelica M, DeMatteo RP, Fong Y, Blumgart LH, et al. Differential diagnosis of proximal biliary obstruction. Surgery. 2006;140:756–63. - PubMed
-
- Binkley CE, Eckhauser FE, Colletti LM. Unusual causes of benign biliary strictures with cholangiographic features of cholangiocarcinoma. J Gastrointest Surg. 2002;6:676–81. - PubMed
LinkOut - more resources
Full Text Sources
