

Cholangiocarcinoma: preoperative biliary drainage (Con)
- PMID: 18773089
- PMCID: PMC2504392
- DOI: 10.1080/13651820802007472
Cholangiocarcinoma: preoperative biliary drainage (Con)
Abstract
Aim: In patients with malignant hilar obstruction, liver resection is associated with an increased risk of postoperative liver failure attributed to the need for major liver resection in a context of obstructive jaundice. To overcome this issue, most authors recommend preoperative biliary drainage (PBD). However, PBD carries risks of its own, including, primarily, sepsis and, more rarely, tumor seeding, bile peritonitis, and hemobilia. We, unlike most authors, have not used routine PBD before liver resection in jaundiced patients.
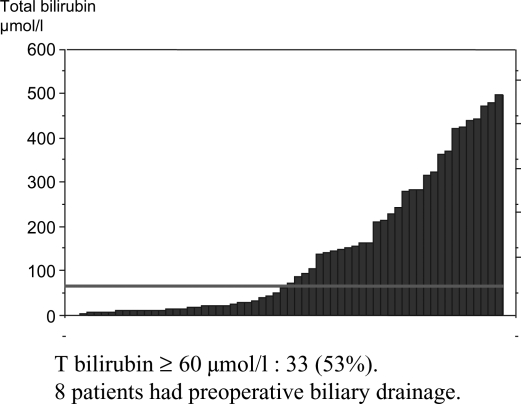
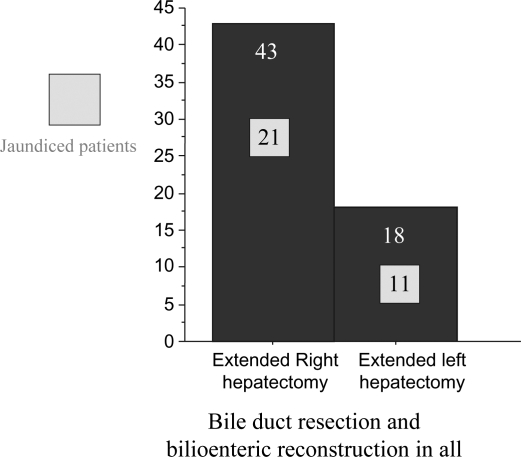
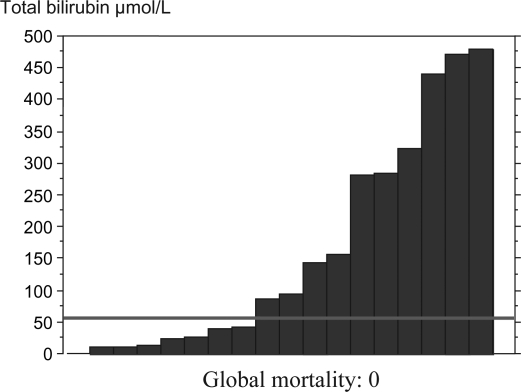
Material and methods: Our series includes 62 patients who underwent major liver resection for cholangiocarcinoma; 33 of these had elevated bilirubin (60-470 micromol/l) and were operated without PBD. There were 43 extended right hepatectomies and 18 extended left hepatectomies.
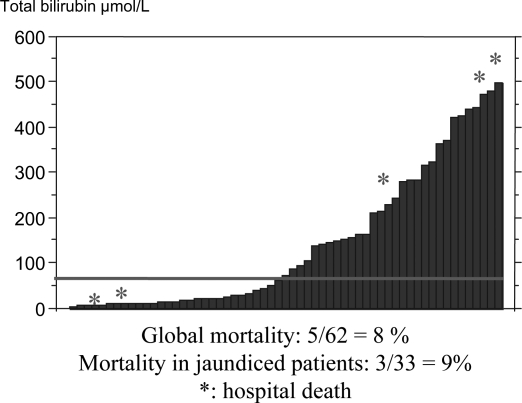
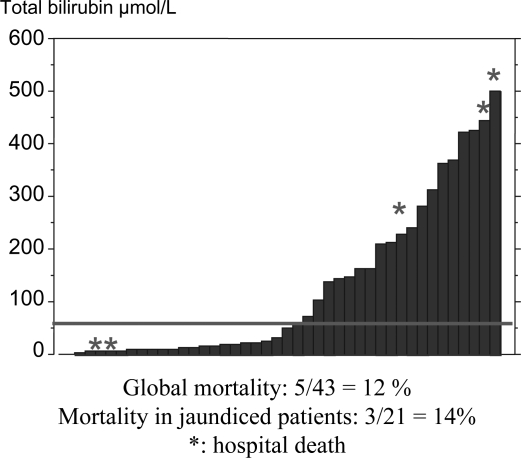
Results: Hospital deaths occurred in 5 patients (8%) including 3 of 33 jaundiced patients (9%, ns). All deaths occurred after extended right hepatectomy (12%), including 3 patients with a serum bilirubin level above 300 micromol/l and 2 with normal bilirubin. There were no deaths after left-sided resections, whatever the level of bilirubin.
Conclusions: PBD can be omitted in the following situations: recent onset jaundice (<2-3 weeks), total bilirubin <200 micromol/l, no previous endoscopic or transhepatic cholangiography, absence of sepsis, future liver remnant >40%. These criteria include most patients requiring left-sided resections and selected patients requiring right-sided resections. In other cases, PBD is required, associated with portal vein embolization in the event of a small future liver remnant.
Figures
References
-
- Nagino M, Nimura Y, Kamiya J, Kondo S, Kanai M, Miyachi M, et al. Preoperative management of hilar cholangiocarcinoma. J Hepatobil Pancreat Surg. 1995;2:215–23.
-
- Miyagawa S, Makuuchi M, Kawasaki S. Outcome of extended right hepatectomy after biliary drainage in hilar bile duct cancer. Arch Surg. 1995;130:759–63. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
