

Laparoscopic liver resection: when to use the laparoscopic stapler device
- PMID: 18773113
- PMCID: PMC2518309
- DOI: 10.1080/13651820802166773
Laparoscopic liver resection: when to use the laparoscopic stapler device
Abstract
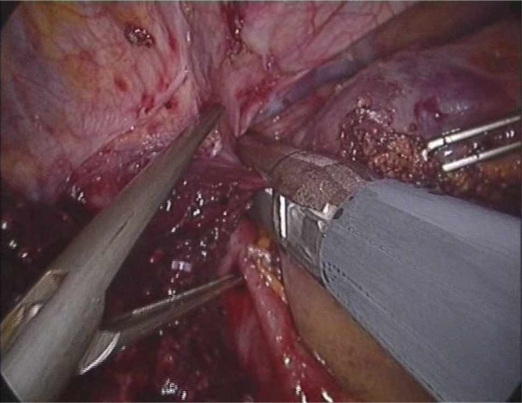
Minimally invasive hepatic resection was first described by Gagner et al. in the early 1990s and since then has become increasingly adopted by hepatobiliary and liver transplant surgeons. Several techniques exist to transect the hepatic parenchyma laparoscopically and include transection with stapler and/or energy devices, such as ultrasonic shears, radiofrequency ablation and bipolar devices. We believe that coagulative techniques allow for superior anatomic resections and ultimately permit for the performance of more complex hepatic resections. In the stapling technique, Glisson's capsule is usually incised with an energy device until the parenchyma is thinned out and multiple firings of the staplers are then used to transect the remaining parenchyma and larger bridging segmental vessels and ducts. Besides the economic constraints of using multiple stapler firings, the remaining staples have the disadvantage of hindering and even preventing additional hemostasis of the raw liver surface with monopolar and bipolar electrocautery. The laparoscopic stapler device is, however, useful for transection of the main portal branches and hepatic veins during minimally invasive major hepatic resections. Techniques to safely perform major hepatic resection with the above techniques will be described with an emphasis on when and how laparoscopic vascular staplers should be used.
Keywords: benign; hepatic; laparoscopic; major; malignant; minor; resection; stapler; stapling technique.
Figures
Similar articles
-
Laparoscopic right hepatectomy with intrahepatic transection of the right bile duct.Ann Surg Oncol. 2012 Feb;19(2):467-8. doi: 10.1245/s10434-011-1927-5. Epub 2011 Aug 6. Ann Surg Oncol. 2012. PMID: 21822559
-
Hepatic resection using stapling devices.Am J Surg. 2004 Feb;187(2):280-4. doi: 10.1016/j.amjsurg.2003.11.005. Am J Surg. 2004. PMID: 14769320
-
Application of stapling devices in liver surgery: Current status and future prospects.World J Gastroenterol. 2016 Aug 21;22(31):7091-8. doi: 10.3748/wjg.v22.i31.7091. World J Gastroenterol. 2016. PMID: 27610019 Free PMC article. Review.
-
The role of the ultrasonically activated shears and vascular cutting stapler in hepatic resection.Am Surg. 2000 Nov;66(11):1037-40. Am Surg. 2000. PMID: 11090014
-
What is the best technique in parenchymal transection in laparoscopic liver resection? Comprehensive review for the clinical question on the 2nd International Consensus Conference on Laparoscopic Liver Resection.J Hepatobiliary Pancreat Sci. 2015 May;22(5):363-70. doi: 10.1002/jhbp.216. Epub 2015 Jan 29. J Hepatobiliary Pancreat Sci. 2015. PMID: 25631462 Review.
Cited by
-
Evaluation of stapler hepatectomy during a laparoscopic liver resection.HPB (Oxford). 2013 Nov;15(11):845-50. doi: 10.1111/hpb.12043. Epub 2013 Jan 18. HPB (Oxford). 2013. PMID: 23458439 Free PMC article.
-
Adopting Gayet's Techniques of Totally Laparoscopic Liver Surgery in the United States.Liver Cancer. 2013 Jan;2(1):5-15. doi: 10.1159/000346213. Liver Cancer. 2013. PMID: 24159591 Free PMC article. Review.
-
Current status of laparoscopic liver resection in Korea.J Korean Med Sci. 2012 Jul;27(7):767-71. doi: 10.3346/jkms.2012.27.7.767. Epub 2012 Jun 29. J Korean Med Sci. 2012. PMID: 22787372 Free PMC article.
-
Milestones in the evolution of hepatic surgery.Rambam Maimonides Med J. 2011 Jan 31;2(1):e0021. doi: 10.5041/RMMJ.10021. Print 2011 Jan. Rambam Maimonides Med J. 2011. PMID: 23908793 Free PMC article.
-
Minireview on laparoscopic hepatobiliary and pancreatic surgery.World J Gastrointest Endosc. 2014 Mar 16;6(3):60-7. doi: 10.4253/wjge.v6.i3.60. World J Gastrointest Endosc. 2014. PMID: 24634709 Free PMC article. Review.
References
-
- Gumbs AA, Gayet B. The laparoscopic duodenopancreatectomy: the posterior approach. Surg Endosc. 2008;22(2):539–540. - PubMed
-
- Gumbs AA, Gres P, Madureira FA, Gayet B. Laparoscopic vs. open resection of noninvasive intraductal pancreatic mucinous neoplasms. J Gastrointest Surg. 2008;12:707–12. - PubMed
-
- Vibert E, Perniceni T, Levard H, Denet C, Shahri NK, Gayet B. Laparoscopic liver resection. Br J Surg. 2006;93(1):67–72. - PubMed
-
- Simillis C, Constantinides VA, Tekkis PP, Darzi A, Lovegrove R, Jiao L, et al. Laparoscopic versus open hepatic resections for benign and malignant neoplasms – a meta-analysis. Surgery. 2007;141(2):203–11. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
