

Importance of socioeconomic status as a predictor of cardiovascular outcome and costs of care in women with suspected myocardial ischemia. Results from the National Institutes of Health, National Heart, Lung and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE)
- PMID: 18774893
- PMCID: PMC2818766
- DOI: 10.1089/jwh.2007.0596
Importance of socioeconomic status as a predictor of cardiovascular outcome and costs of care in women with suspected myocardial ischemia. Results from the National Institutes of Health, National Heart, Lung and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE)
Abstract
Background: For women, who are more likely to live in poverty, defining the clinical and economic impact of socioeconomic factors may aid in defining redistributive policies to improve healthcare quality.
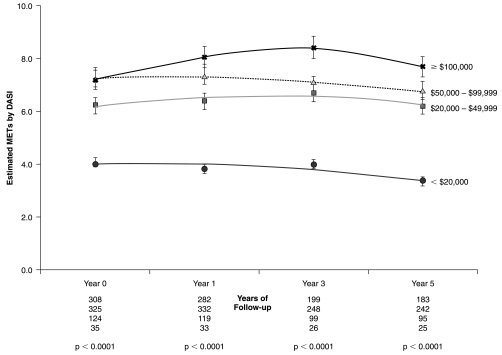
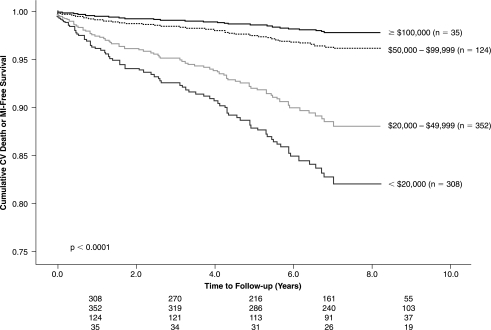
Methods: The NIH-NHLBI-sponsored Women's Ischemia Syndrome Evaluation (WISE) enrolled 819 women referred for clinically indicated coronary angiography. This study's primary end point was to evaluate the independent contribution of socioeconomic factors on the estimation of time to cardiovascular death or myocardial infarction (MI) (n = 79) using Cox proportional hazards models. Secondary aims included an examination of cardiovascular costs and quality of life within socioeconomic subsets of women.
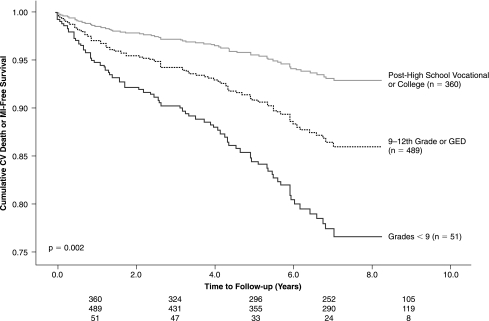
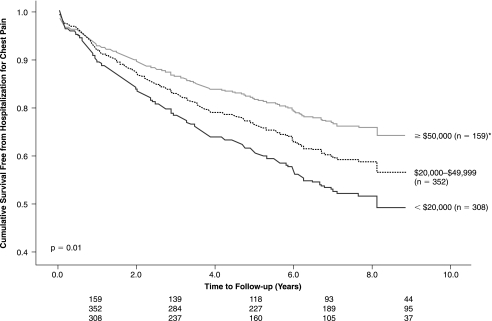
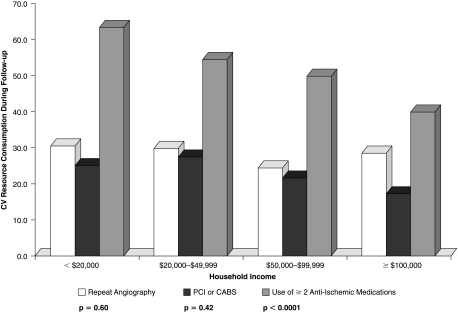
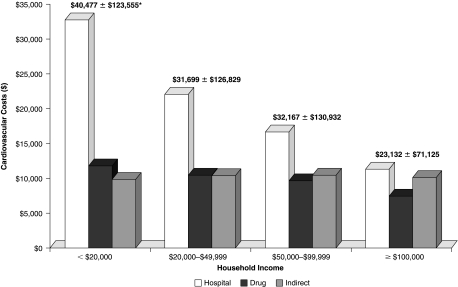
Results: In univariable models, socioeconomic factors associated with an elevated risk of cardiovascular death or MI included an annual household income <$20,000 (p = 0.0001), <9th grade education (p = 0.002), being African American, Hispanic, Asian, or American Indian (p = 0.016), on Medicaid, Medicare, or other public health insurance (p < 0.0001), unmarried (p = 0.001), unemployed or employed part-time (p < 0.0001), and working in a service job (p = 0.003). Of these socioeconomic factors, income (p = 0.006) remained a significant predictor of cardiovascular death or MI in risk-adjusted models that controlled for angiographic coronary disease, chest pain symptoms, and cardiac risk factors. Low-income women, with an annual household income <$20,000, were more often uninsured or on public insurance (p < 0.0001) yet had the highest 5-year hospitalization and drug treatment costs (p < 0.0001). Only 17% of low-income women had prescription drug coverage (vs. >or=50% of higher-income households, p < 0.0001), and 64% required >or=2 anti-ischemic medications during follow-up (compared with 45% of those earning >or=$50,000, p < 0.0001).
Conclusions: Economic disadvantage prominently affects cardiovascular disease outcomes for women with chest pain symptoms. These results further support a profound intertwining between poverty and poor health. Cardiovascular disease management strategies should focus on policies that track unmet healthcare needs and worsening clinical status for low-income women.
Figures
Similar articles
-
Depressive symptom dimensions and cardiovascular prognosis among women with suspected myocardial ischemia: A report from the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation.Arch Gen Psychiatry. 2009 May;66(5):499-507. doi: 10.1001/archgenpsychiatry.2009.27. Arch Gen Psychiatry. 2009. PMID: 19414709 Free PMC article.
-
Self-rated versus objective health indicators as predictors of major cardiovascular events: the NHLBI-sponsored Women's Ischemia Syndrome Evaluation.Psychosom Med. 2010 Jul;72(6):549-55. doi: 10.1097/PSY.0b013e3181dc0259. Epub 2010 Apr 21. Psychosom Med. 2010. PMID: 20410246 Free PMC article.
-
Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: results from the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women's Ischemia Syndrome Evaluation (WISE).Circulation. 2004 Jun 22;109(24):2993-9. doi: 10.1161/01.CIR.0000130642.79868.B2. Epub 2004 Jun 14. Circulation. 2004. PMID: 15197152
-
Even "WISE-R?"-an Update on the NHLBI-Sponsored Women's Ischemia Syndrome Evaluation.Curr Atheroscler Rep. 2020 Jun 18;22(8):35. doi: 10.1007/s11883-020-00852-w. Curr Atheroscler Rep. 2020. PMID: 32556630 Free PMC article. Review.
-
Stable angina in women: lessons from the National Heart, Lung and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation.J Cardiovasc Med (Hagerstown). 2011 Feb;12(2):85-7. doi: 10.2459/JCM.0b013e3283430969. J Cardiovasc Med (Hagerstown). 2011. PMID: 21228716 Review.
Cited by
-
Racial/Ethnic Differences in Cardiovascular Symptoms in Four Major Racial/Ethnic Groups of Midlife Women: A Secondary Analysis.Women Health. 2015;55(5):525-47. doi: 10.1080/03630242.2015.1022813. Epub 2015 Mar 31. Women Health. 2015. PMID: 25826460 Free PMC article.
-
Awareness of cardiovascular disease among Korean women: Results from a nationwide survey.Prev Med Rep. 2022 Jan 19;26:101698. doi: 10.1016/j.pmedr.2022.101698. eCollection 2022 Apr. Prev Med Rep. 2022. PMID: 35111568 Free PMC article.
-
Clinical practice guideline of the Interamerican Society of Cardiology on primary prevention of cardiovascular disease in women.Arch Cardiol Mex. 2022;92(Supl 2):1-68. doi: 10.24875/ACM.22000071. Arch Cardiol Mex. 2022. PMID: 35666723 Free PMC article. English. No abstract available.
-
Assessment of distance to primary percutaneous coronary intervention centres in ST-segment elevation myocardial infarction: Overcoming inequalities with process mining tools.Digit Health. 2023 Jan 17;9:20552076221144210. doi: 10.1177/20552076221144210. eCollection 2023 Jan-Dec. Digit Health. 2023. PMID: 36698425 Free PMC article.
-
Managing Ischemic Heart Disease in Women: Role of a Women's Heart Center.Curr Atheroscler Rep. 2021 Aug 4;23(10):56. doi: 10.1007/s11883-021-00956-x. Curr Atheroscler Rep. 2021. PMID: 34345945 Free PMC article. Review.
References
-
- Marmot MG. Shipley MJ. Rose G. Inequalities in death-specific explanations of a general pattern. Lancet. 1984;1:1003–1006. - PubMed
-
- Steenland K. Henley J. Calle E. Thun M. Individual- and area-level socioeconomic status variables as predictors of mortality in a cohort of 179,383 persons. Am J Epidemiol. 2004;159:1047–1056. - PubMed
-
- Kaplan GA. Keil JE. Socioeconomic factors and cardiovascular disease: A review of the literature. Circulation. 1995;88:1973–1998. - PubMed
-
- Feinstein JS. The relationship between socioeconomic status and health: A review of the literature. Milbank Q. 1993;71:279–322. - PubMed
-
- Syme SL. Berkman LF. Social class, susceptibility and sickness. Am J Epidemiol. 1976;104:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
