

Evidence of a causal role of winter virus infection during infancy in early childhood asthma
- PMID: 18776151
- PMCID: PMC2588491
- DOI: 10.1164/rccm.200804-579OC
Evidence of a causal role of winter virus infection during infancy in early childhood asthma
Abstract
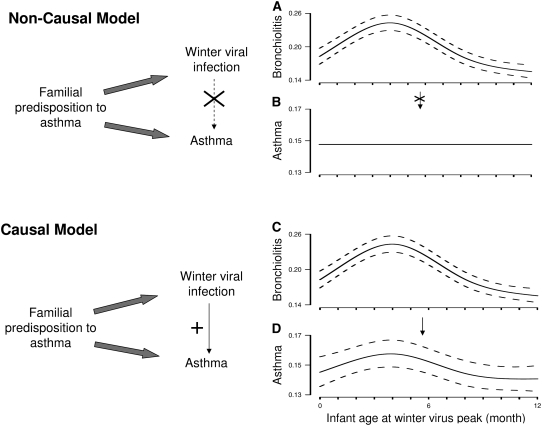
Rationale: Bronchiolitis during infancy is associated with an increased risk of childhood asthma. Whether winter viral infections cause asthma or are a manifestation of a predisposition to asthma development is unknown.
Objectives: To study the relationship of winter virus infection during infancy and the development of childhood asthma.
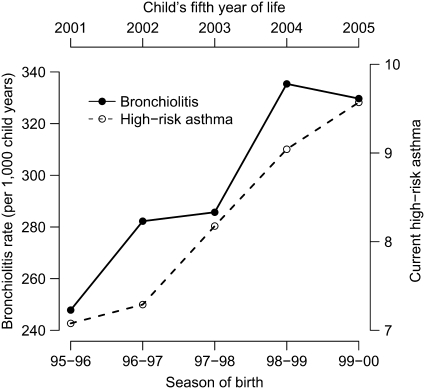
Methods: We studied over 95,000 infants born between 1995 and 2000 and followed through 2005 who were enrolled in the Tennessee Medicaid program from birth through early childhood to determine whether infant birth in relationship to the winter virus peak alters the risk of developing early childhood asthma.
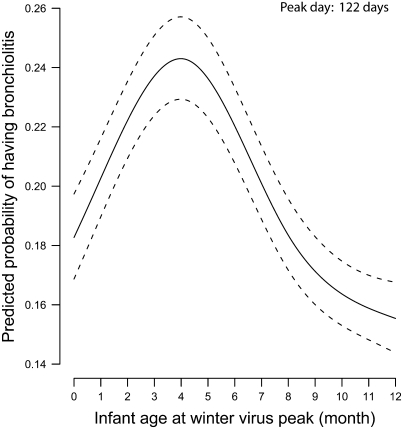
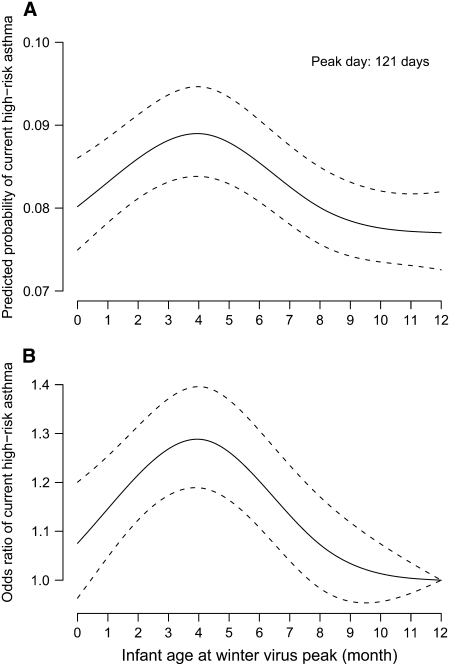
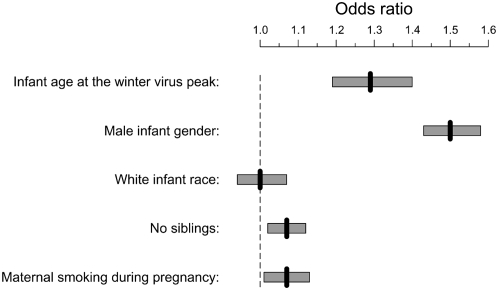
Measurements and main results: Among 95,310 children studied during five winter virus seasons from birth through early childhood, the risk of developing asthma tracked with the timing of infant birth in relationship to the winter virus peak. Infant birth approximately 4 months before the winter virus peak carried the highest risk, with a 29% increase in odds of developing asthma compared with birth 12 months before the peak (adjusted odds ratio, 1.29; 95% confidence interval, 1.19-1.40). Infant age at the winter virus peak was comparable to or greater than other known risk factors for asthma.
Conclusions: Timing of birth in relationship to winter virus season confers a differential and definable risk of developing early childhood asthma, establishing winter virus seasonality as a causal factor in asthma development. Delay of exposure or prevention of winter viral infection during early infancy could prevent asthma.
Figures
Comment in
-
Early-life viral bronchiolitis in the causal pathway of childhood asthma: is the evidence there yet?Am J Respir Crit Care Med. 2008 Dec 1;178(11):1097-8. doi: 10.1164/rccm.200808-1305ED. Am J Respir Crit Care Med. 2008. PMID: 19023035 No abstract available.
-
The roles of vitamin D, temperature, and viral infections in seasonal risk of acquiring asthma.Am J Respir Crit Care Med. 2009 Jun 1;179(11):1072; author reply 1072-3. doi: 10.1164/ajrccm.179.11.1072. Am J Respir Crit Care Med. 2009. PMID: 19458272 No abstract available.
References
-
- Asthma Facts from WHO Statistical Information System WHOSIS [accessed June 22, 2008]. Available from: http://www.who.int/respiratory/asthma/en
-
- Sigurs N, Bjarnason R, Sigurbergsson F, Kjellman B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am J Respir Crit Care Med 2000;161:1501–1507. - PubMed
-
- Sigurs N, Gustafsson PM, Bjarnason R, Lundberg F, Schmidt S, Sigurbergsson F, Kjellman B. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am J Respir Crit Care Med 2005;171:137–141. - PubMed
-
- Henderson J, Hilliard TN, Sherriff A, Stalker D, Al Shammari N, Thomas HM. Hospitalization for RSV bronchiolitis before 12 months of age and subsequent asthma, atopy and wheeze: a longitudinal birth cohort study. Pediatr Allergy Immunol 2005;16:386–392. - PubMed
