

The 3 H and BMSEST models for spirituality in multicultural whole-person medicine
- PMID: 18779550
- PMCID: PMC2532766
- DOI: 10.1370/afm.864
The 3 H and BMSEST models for spirituality in multicultural whole-person medicine
Abstract
Purpose: The explosion of evidence in the last decade supporting the role of spirituality in whole-person patient care has prompted proposals for a move to a biopsychosocial-spiritual model for health. Making this paradigm shift in today's multicultural societies poses many challenges, however. This article presents 2 theoretical models that provide common ground for further exploration of the role of spirituality in medicine.
Methods: The 3 H model (head, heart, hands) and the BMSEST models (body, mind, spirit, environment, social, transcendent) evolved from the author's 12-year experience with curricula development regarding spirituality and medicine, 16-year experience as an attending family physician and educator, lived experience with both Hinduism and Christianity since childhood, and a lifetime study of the world's great spiritual traditions. The models were developed, tested with learners, and refined.
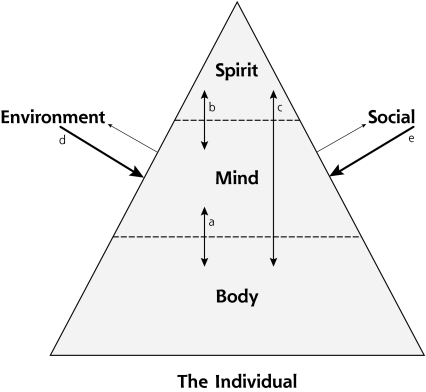
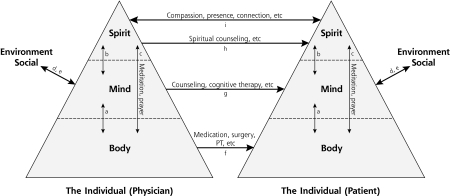
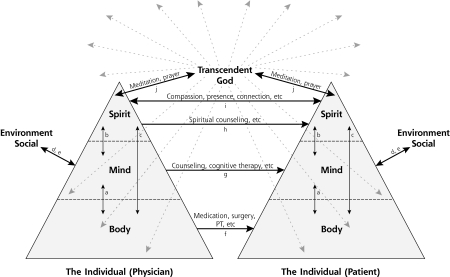
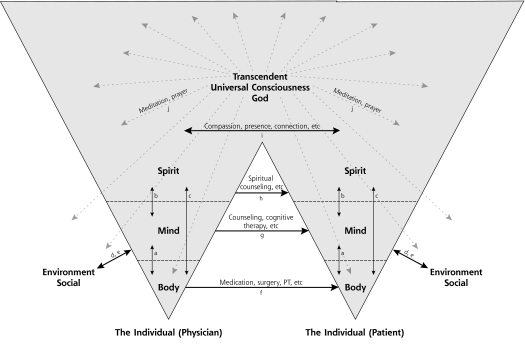
Results: The 3 H model offers a multidimensional definition of spirituality, applicable across cultures and belief systems, that provides opportunities for a common vocabulary for spirituality. Therapeutic options, from general spiritual care (compassion, presence, and the healing relationship), to specialized spiritual care (eg, by clinical chaplains), to spiritual self-care are discussed. The BMSEST model provides a conceptual framework for the role of spirituality in the larger health care context, useful for patient care, education, and research. Interactions among the 6 BMSEST components, with references to ongoing research, are proposed.
Conclusions: Including spirituality in whole-person care is a way of furthering our understanding of the complexities of human health and well-being. The 3 H and BMSEST models suggest a multidimensional and multidisciplinary approach based on universal concepts and a foundation in both the art and science of medicine.
Figures
Comment in
-
Spirituality and medicine: science and practice.Ann Fam Med. 2008 Sep-Oct;6(5):388-9. doi: 10.1370/afm.900. Ann Fam Med. 2008. PMID: 18779541 Free PMC article. No abstract available.
Similar articles
-
Map of the spirit: Diagnosis and treatment of spiritual disease.Adv Mind Body Med. 2008 Summer;23(2):6-16. Adv Mind Body Med. 2008. PMID: 20664140
-
Medicine and spirituality: a simple path to restore compassion in medicine.S D J Med. 2002 Nov;55(11):487-91. S D J Med. 2002. PMID: 12449590 Review.
-
Reevaluation of a nursing diagnosis: spiritual distress.Nurs Forum. 1992 Oct-Dec;27(4):15-20. doi: 10.1111/j.1744-6198.1992.tb00914.x. Nurs Forum. 1992. PMID: 1470529
-
A 10-Year Longitudinal Study of Effects of a Multifaceted Residency Spiritual Care Curriculum: Clinical Ability, Professional Formation, End of Life, and Culture.J Pain Symptom Manage. 2016 Dec;52(6):859-872.e1. doi: 10.1016/j.jpainsymman.2016.06.006. Epub 2016 Oct 3. J Pain Symptom Manage. 2016. PMID: 27713033
-
Spiritual care for sick children of five world faiths.Paediatr Nurs. 2006 Dec;18(10):22-5. doi: 10.7748/paed.18.10.22.s18. Paediatr Nurs. 2006. PMID: 17193915 Review.
Cited by
-
Along the way to developing a theory of the program: a re-examination of the conceptual framework as an organizing strategy.Eval Program Plann. 2014 Aug;45:157-63. doi: 10.1016/j.evalprogplan.2014.04.005. Epub 2014 Apr 30. Eval Program Plann. 2014. PMID: 24836998 Free PMC article.
-
A model for the role of defined spirituality in South African specialist psychiatric practice and training.J Relig Health. 2014 Apr;53(2):393-412. doi: 10.1007/s10943-012-9644-3. J Relig Health. 2014. PMID: 23099614
-
Defining and Measuring Spirituality in South African Specialist Psychiatry.J Relig Health. 2015 Oct;54(5):1839-55. doi: 10.1007/s10943-014-9943-y. J Relig Health. 2015. PMID: 25266141
-
Religion and Spirituality in Lifestyle Medicine.Am J Lifestyle Med. 2024 Aug 29;19(2):324-333. doi: 10.1177/15598276241276770. eCollection 2025 Feb. Am J Lifestyle Med. 2024. PMID: 39554923 Free PMC article. Review.
-
Defining Spirituality in Healthcare: A Systematic Review and Conceptual Framework.Front Psychol. 2021 Nov 18;12:756080. doi: 10.3389/fpsyg.2021.756080. eCollection 2021. Front Psychol. 2021. PMID: 34867654 Free PMC article.
References
-
- Lown B. The Lost Art of Healing. New York, NY: Ballantine Books; 1999.
-
- Murray CJ, Lopez AD. Global mortality, disability and the contribution of risk factors: global burden of disease study. Lancet. 1997;349(9063):1436–1442. - PubMed
-
- Benson H, Malvea BP, Graham JR. Psysiologic correlates of meditation and their clinical effects in headache: an ongoing investigation. Headache. 1973;13(1):23–24. - PubMed
-
- Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation. Gen Hosp Psychiatry. 1982;4(1):33–47. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources