

Lymphovascular invasion in colorectal cancer: an interobserver variability study
- PMID: 18779725
- PMCID: PMC2605104
- DOI: 10.1097/PAS.0b013e3181816083
Lymphovascular invasion in colorectal cancer: an interobserver variability study
Abstract
Background: Lymphovascular invasion (LVI) in colorectal cancer (CRC) is considered a strong stage-independent prognostic factor and influences decisions regarding adjuvant chemotherapy in patients with stage II tumors. However, the degree of interobserver agreement among pathologists for LVI in CRC is largely unknown. This study was undertaken to examine such interobserver variability, and we hypothesized that the use of immunohistochemical markers for vascular and lymphatic channels could improve interobserver agreement.
Design: Fifty cases of American Joint Committee on Cancer stage II moderately differentiated CRC from 1990 to 2005 from the pathology archives were selected; mucinous, medullary, and other recognized special subtypes were excluded. Fifty hematoxylin and eosin (H&E) slides (1 from each case) were circulated to 6 gastrointestinal pathologists, who independently assessed small and large vessel invasion. No diagnostic guidelines were given to the participating pathologists; each was instructed to apply the criteria for LVI that he or she used in daily practice. Immunohistochemistry (IHC) for D2-40 and CD31 was performed on corresponding paraffin blocks. The IHC slides were randomized, recirculated, and rescored for LVI. Results were analyzed by kappa (kappa) statistics, which correct for agreement by chance, and for percentage agreement.
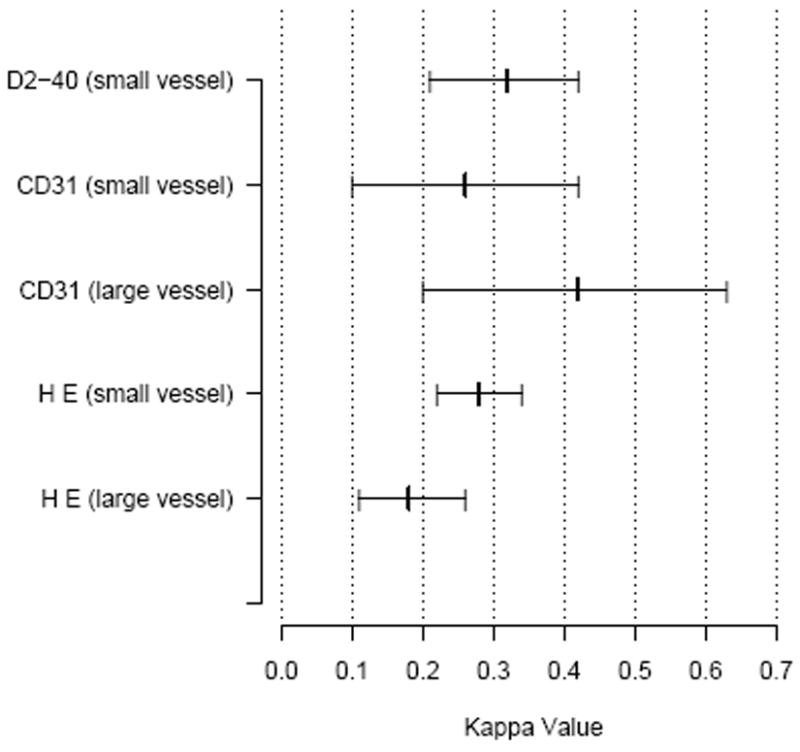
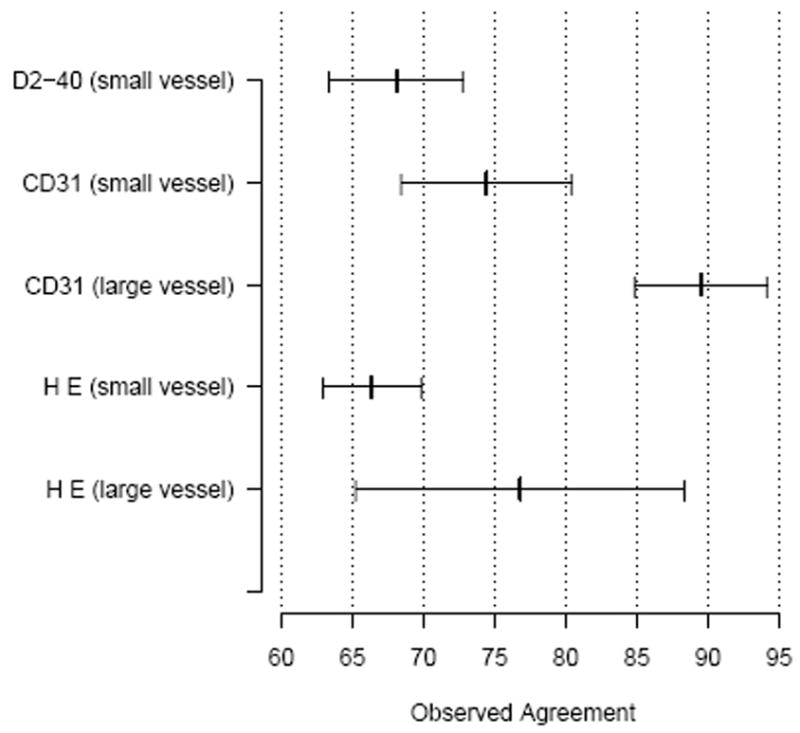
Results: The average kappa values were determined for the H&E slides (large and small vessel), CD31 (small vessel), and D2-40 (small vessel) (Fig. 1). Agreement was fair for H&E small vessel invasion [kappa=0.28; 95% confidence interval (CI): 0.22-0.34]. The least agreement was seen in interpretation of H&E large vessel invasion (kappa=0.18; 95%CI: 0.11-0.26). Agreement was not improved by use of immunohistochemical stains: CD31 (large vessel, kappa=0.42, 95%CI: 0.20-0.63, small vessel, kappa=0.26, 95%CI: 0.10-0.42) and D2-40 (kappa=0.32, 95%CI: 0.21-0.42).
Conclusions: Interobserver variability in diagnosis of LVI was substantial on H&E slides and did not improve upon use of IHC. Agreement in evaluation of large vessel invasion was only slightly higher than would be seen by chance alone. This study highlights the need for criteria in evaluation of LVI, as this assessment may impact patient prognosis and thus change the course of clinical treatment.
Figures
Similar articles
-
Lymphovascular invasion in early gastric cancer: impact of ancillary D2-40 and elastin staining on interobserver agreement.Histopathology. 2020 May;76(6):888-897. doi: 10.1111/his.14075. Epub 2020 May 3. Histopathology. 2020. PMID: 31989674
-
ERG Immunohistochemistry as an Endothelial Marker for Assessing Lymphovascular Invasion.Korean J Pathol. 2013 Aug;47(4):355-64. doi: 10.4132/KoreanJPathol.2013.47.4.355. Epub 2013 Aug 26. Korean J Pathol. 2013. PMID: 24009631 Free PMC article.
-
Interobserver Agreement in Vascular Invasion Scoring and the Added Value of Immunohistochemistry for Vascular Markers to Predict Disease Relapse in Stage I Testicular Nonseminomas.Am J Surg Pathol. 2019 Dec;43(12):1711-1719. doi: 10.1097/PAS.0000000000001352. Am J Surg Pathol. 2019. PMID: 31490238
-
The Usefulness of Elastin Staining to Detect Vascular Invasion in Cancer.Int J Mol Sci. 2023 Oct 17;24(20):15264. doi: 10.3390/ijms242015264. Int J Mol Sci. 2023. PMID: 37894944 Free PMC article. Review.
-
Additional staining for lymphovascular invasion is associated with increased estimation of lymph node metastasis in patients with T1 colorectal cancer: Systematic review and meta-analysis.Dig Endosc. 2024 May;36(5):533-545. doi: 10.1111/den.14691. Epub 2023 Oct 25. Dig Endosc. 2024. PMID: 37746764 Free PMC article.
Cited by
-
Ensemble Deep Learning Model to Predict Lymphovascular Invasion in Gastric Cancer.Cancers (Basel). 2024 Jan 19;16(2):430. doi: 10.3390/cancers16020430. Cancers (Basel). 2024. PMID: 38275871 Free PMC article.
-
The Prognostic Reliability of Lymphovascular Invasion for Patients with T3N0 Colorectal Cancer in Adjuvant Chemotherapy Decision Making.Cancers (Basel). 2022 Jun 8;14(12):2833. doi: 10.3390/cancers14122833. Cancers (Basel). 2022. PMID: 35740498 Free PMC article.
-
Preoperative prediction of the lymphovascular tumor thrombus of colorectal cancer with the iodine concentrations from dual-energy spectral CT.BMC Med Imaging. 2023 Aug 3;23(1):103. doi: 10.1186/s12880-023-01060-z. BMC Med Imaging. 2023. PMID: 37537532 Free PMC article.
-
Effect of skip lymphovascular invasion on hepatic metastasis in colorectal carcinomas.Int J Clin Oncol. 2015 Aug;20(4):761-6. doi: 10.1007/s10147-014-0778-z. Epub 2014 Dec 9. Int J Clin Oncol. 2015. PMID: 25483315
-
Histology-based prediction of lymph node metastases in early gastric cancer as decision guidance for endoscopic resection.Oncotarget. 2016 Mar 1;7(9):10676-83. doi: 10.18632/oncotarget.7221. Oncotarget. 2016. PMID: 26863452 Free PMC article.
References
-
- Brodsky JT, Richard GK, Cohen AM, et al. Variables correlated with the risk of lymph node metastasis in early rectal cancer. Cancer. 1992;69:322–6. - PubMed
-
- Compton C, Fenoglio-Preiser CM, Pettigrew N, et al. American Joint Committee on Cancer Prognostic Factors Consensus Conference: Colorectal Working Group. Cancer. 2000 Apr 1;88(7):1739–57. - PubMed
-
- Compton CC. Key issues in reporting common cancer specimens: problems in pathologic staging of colon cancer. Arch Pathol Lab Med. 2006;130(3):318–24. - PubMed
-
- Compton CC, Fielding LP, Burgart LJ, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med. 2000;124(7):979–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
