

Posterior approach for double nerve transfer for restoration of shoulder function in upper brachial plexus palsy
- PMID: 18780028
- PMCID: PMC2526027
- DOI: 10.1007/s11552-006-9004-4
Posterior approach for double nerve transfer for restoration of shoulder function in upper brachial plexus palsy
Abstract
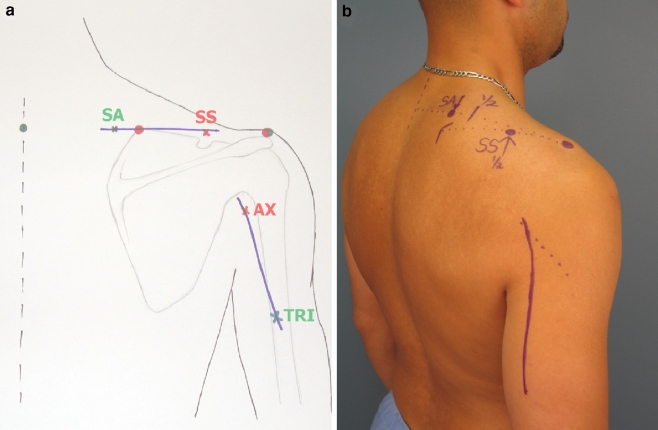
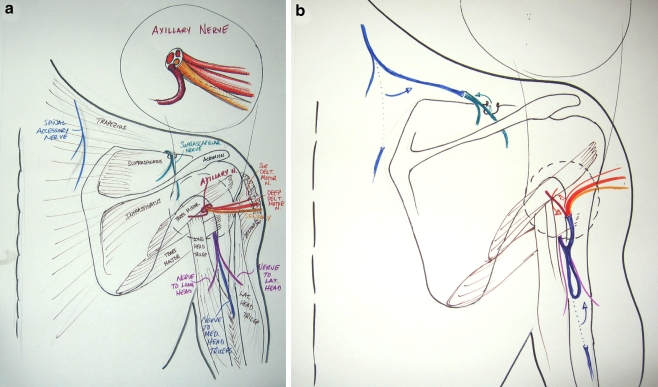
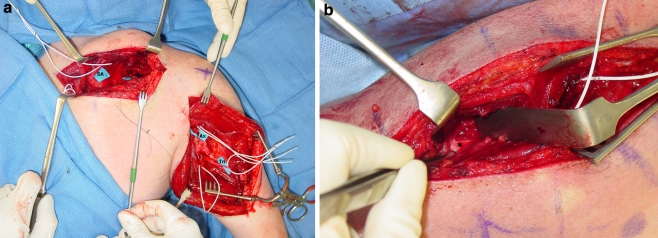
Restoration of shoulder function is one of the most critical goals of treatment of brachial plexus injuries. Primary repair or nerve grafting of avulsion injuries of the upper brachial plexus in adults often leads to poor recovery. Nerve transfers have provided an alternative treatment with great potential for improved return of function. Many different nerves have been utilized as donor nerves for transfer to the suprascapular nerve and axillary nerve for return of shoulder function with variable results. As our knowledge of shoulder neuromuscular anatomy and physiology improves and our experience with nerve transfers increases, so evolve the specific transfer procedures. This article presents a technique and rationale for reconstructing shoulder function by transferring the distal spinal accessory nerve to the suprascapular nerve and the nerve branch to the medial head of the triceps to the axillary nerve, both through a posterior approach.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '15622257', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15622257/'}]}
- Bahm J, Naoman H, Becker M. The dorsal approach to the suprascapular nerve in neuromuscular reanimation for obstetric brachial plexus lesions. Plast Reconstr Surg 2005;115:240–4. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '14751116', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14751116/'}]}
- Bertelli JA, Ghizoni MF. Reconstruction of C5 and C6 brachial plexus avulsion injury by multiple nerve transfers: spinal accessory to suprascapular, ulnar fascicles to biceps branch, and triceps long or lateral head branch to axillary nerve. J Hand Surg 2004;29A:131–9. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '16582662', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16582662/'}]}
- Bertelli JA, Ghizoni MF. Improved technique for harvesting the accessory nerve for transfer in brachial plexus injuries. Neurosurgery 2006;58(4) Suppl 2:ONS-366-70; discussion ONS-370. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC6569224', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC6569224/'}, {'type': 'PubMed', 'value': '3346713', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/3346713/'}]}
- Brushart TME. Preferential reinnervation of motor nerves by regenerating motor axons. J Neurosci 1988;8:1026–31. - PMC - PubMed
-
- None
- Celli L, Rovesta C, Balli A. Neurotization of brachial plexus avulsion with intercostal nerves (personal techniques). In: Brunelli G, editor. Textbook of microsurgery. Milano: Masson; 1988. p. 789–95.
LinkOut - more resources
Full Text Sources
Research Materials
