

Management of recurrent carpal tunnel syndrome with microneurolysis and the hypothenar fat pad flap
- PMID: 18780064
- PMCID: PMC2527148
- DOI: 10.1007/s11552-007-9025-7
Management of recurrent carpal tunnel syndrome with microneurolysis and the hypothenar fat pad flap
Abstract
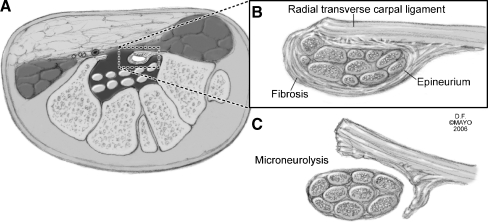
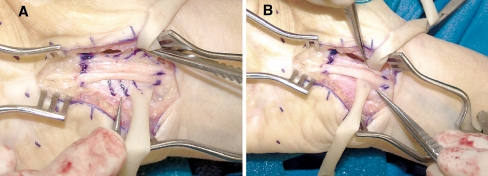
A retrospective chart review for the period between 1998 and 2006 was conducted to evaluate microneurolysis combined with a hypothenar fat pad flap (HTFPF) for patients at Mayo Clinic, Scottsdale, Arizona, who were being treated for recurrent carpal tunnel syndrome. After exclusion of patients with incomplete release of the transverse carpal ligament at the time of the original operation, 28 consecutive patients were identified. Their average age was 68.5 years (range 43-89 years). The average interval between the original carpal tunnel release and reexploration was 82 months (range 5-298 months). The average follow-up was 10.5 months (range 3-48.4 months). The preoperative two-point discrimination tests averaged 7 mm (range 5-12 mm). At surgery, all patients were found to have fibrosis surrounding the median nerve with adherence of the nerve to the radial leaf of the transverse carpal ligament. After surgery, the Tinel sign disappeared in 26 of 28 patients and two-point discrimination improved to an average of 6 mm (range 4-8 mm). Postoperative grip strength averaged 20 kg, compared with 11 kg preoperatively. Pain completely disappeared in 83% of patients (average improvement 93%, range 5-100%). Numbness completely disappeared in 42% of patients (average improvement 82.9%, range 5-100%). Tingling disappeared in 50% of patients (average improvement 84.7%, range 5-100%). No patient reported being worse after reoperation. These results suggest that the combination of microneurolysis and HTFPF can restore median nerve gliding and provide soft-tissue coverage, improving symptoms in patients with recurrent carpal tunnel syndrome.
Figures

Similar articles
-
Hypothenar fat pad flap vs conventional open release in primary carpal tunnel syndrome: A randomized controlled trial.World J Orthop. 2017 Nov 18;8(11):846-852. doi: 10.5312/wjo.v8.i11.846. eCollection 2017 Nov 18. World J Orthop. 2017. PMID: 29184759 Free PMC article.
-
Vascularized Hypothenar Fat Pad Flap in Revision Surgery for Carpal Tunnel Syndrome.J Neurol Surg A Cent Eur Neurosurg. 2015 Nov;76(6):438-42. doi: 10.1055/s-0035-1551831. Epub 2015 Jul 27. J Neurol Surg A Cent Eur Neurosurg. 2015. PMID: 26216740
-
[Surgical treatment of carpal tunnel syndrome: open release of the flexor retinaculum and hypothenar fat flap for revision surgery].Oper Orthop Traumatol. 2020 Jun;32(3):219-235. doi: 10.1007/s00064-020-00662-y. Epub 2020 Jun 10. Oper Orthop Traumatol. 2020. PMID: 32524170 German.
-
Management of Recurrent Carpal Tunnel Syndrome: Systematic Review and Meta-Analysis.J Hand Surg Am. 2022 Apr;47(4):388.e1-388.e19. doi: 10.1016/j.jhsa.2021.05.007. Epub 2021 Aug 3. J Hand Surg Am. 2022. PMID: 34353640
-
The hypothenar fat pad transposition flap: a modified surgical technique.Tech Hand Up Extrem Surg. 2006 Sep;10(3):150-6. doi: 10.1097/01.bth.0000225004.56982.42. Tech Hand Up Extrem Surg. 2006. PMID: 16974219 Review.
Cited by
-
Revision Peripheral Nerve Surgery of the Upper Extremity.Semin Plast Surg. 2021 May;35(2):119-129. doi: 10.1055/s-0041-1727290. Epub 2021 Jun 8. Semin Plast Surg. 2021. PMID: 34121947 Free PMC article. Review.
-
Outcomes following use of VersaWrap nerve protector in treatment of patients with recurrent compressive neuropathies.Front Surg. 2023 Mar 21;10:1123375. doi: 10.3389/fsurg.2023.1123375. eCollection 2023. Front Surg. 2023. PMID: 37025263 Free PMC article.
-
Surgical options for recalcitrant carpal tunnel syndrome with perineural fibrosis.Hand (N Y). 2012 Mar;7(1):23-9. doi: 10.1007/s11552-012-9391-7. Epub 2012 Jan 19. Hand (N Y). 2012. PMID: 23450185 Free PMC article.
-
Hypothenar fat pad flap vs conventional open release in primary carpal tunnel syndrome: A randomized controlled trial.World J Orthop. 2017 Nov 18;8(11):846-852. doi: 10.5312/wjo.v8.i11.846. eCollection 2017 Nov 18. World J Orthop. 2017. PMID: 29184759 Free PMC article.
-
Autologous Fat Transfer in Secondary Carpal Tunnel Release.Plast Reconstr Surg Glob Open. 2015 Jun 5;3(5):e401. doi: 10.1097/GOX.0000000000000374. eCollection 2015 May. Plast Reconstr Surg Glob Open. 2015. PMID: 26090291 Free PMC article.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '3714079', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/3714079/'}]}
- Bloem JJ, Pradjarahardja MC, Vuursteen PJ. The post-carpal tunnel syndrome: causes and prevention. Neth J Surg 1986;38:52–5. - PubMed
-
- Cramer LM. Local fat coverage for the median nerve. ASSH Correspondence Newsletter 1985;35.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5907222', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5907222/'}]}
- Cseuz KA, Thomas JE, Lambert EH, Love JG, Lipscomb PR. Long-term results of operation for carpal tunnel syndrome. Mayo Clin Proc 1966;41:232–41. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/0072-968X(76)90009-7', 'is_inner': False, 'url': 'https://doi.org/10.1016/0072-968x(76)90009-7'}, {'type': 'PubMed', 'value': '976823', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/976823/'}]}
- Das SK, Brown HG. In search of complications in carpal tunnel decompression. Hand 1976;8:243–9. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/0266-7681(93)90105-O', 'is_inner': False, 'url': 'https://doi.org/10.1016/0266-7681(93)90105-o'}, {'type': 'PubMed', 'value': '8501371', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8501371/'}]}
- De Smet L. Recurrent carpal tunnel syndrome: clinical testing indicating incomplete section of the flexor retinaculum. J Hand Surg (Br) 1993;18:189. - PubMed
LinkOut - more resources
Full Text Sources
