

Use of a dual mobility socket to manage total hip arthroplasty instability
- PMID: 18780135
- PMCID: PMC2628522
- DOI: 10.1007/s11999-008-0476-0
Use of a dual mobility socket to manage total hip arthroplasty instability
Abstract
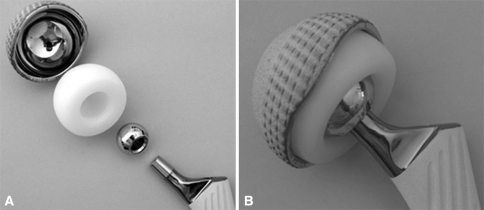
Unconstrained tripolar hip implants provide an additional bearing using a mobile polyethylene component between the prosthetic head and the outer metal shell. Such a design increases the effective head diameter and therefore is an attractive option in challenging situations of unstable total hip arthroplasties. We report our experience with 54 patients treated using this dual mobility implant in such situations. We ascertained its ability to restore and maintain stability, and examined component loosening and component failure. At a minimum followup of 2.2 years (mean, 4 years; range, 2.2-6.8 years), one hip had redislocated 2 months postoperatively and was managed successfully without reoperation by closed reduction with no additional dislocation. Two patients required revision of the implant because of dislocation at the inner bearing. Technical errors were responsible for these failures. Three patients had reoperations for deep infections. The postoperative radiographs at latest followup showed very satisfactory osseointegration of the acetabular component because no radiolucent line or osteolysis was reported. Use of this unconstrained tripolar design was successful in restoring and maintaining hip stability. We observed encouraging results at short-term followup regarding potential for loosening or mechanical failures.
Level of evidence: Level IV, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures

References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '16327667', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16327667/'}]}
- Adam P, Farizon F, Fessy MH. [Dual articulation retentive acetabular liners and wear: surface analysis of 40 retrieved polyethylene implants][in French]. Rev Chir Orthop Reparatrice Appar Mot. 2005;91:627–636. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '7217144', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7217144/'}]}
- Ali Khan MA, Brakenbury PH, Reynolds IS. Dislocation following total hip replacement. J Bone Joint Surg Br. 1981;63:214–218. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/0883-5403(94)90133-3', 'is_inner': False, 'url': 'https://doi.org/10.1016/0883-5403(94)90133-3'}, {'type': 'PubMed', 'value': '8163971', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8163971/'}]}
- Anderson MJ, Murray WR, Skinner HB. Constrained acetabular components. J Arthroplasty. 1994;9:17–23. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '12132797', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12132797/'}]}
- Attarian DE. Bipolar arthroplasty for recurrent total hip instability. J South Orthop Assoc. 1999;8:249–253. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '8116409', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8116409/'}]}
- Aubriot JH, Lesimple P, Leclercq S. [Study of Bousquet’s non-cemented acetabular implant in 100 hybrid total hip prostheses (Charnley type cemented femoral component): average 5-year follow-up][in French]. Acta Orthop Belg. 1993;59(suppl 1):267–271. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
