

Adult gliosarcoma: epidemiology, natural history, and factors associated with outcome
- PMID: 18780813
- PMCID: PMC2718990
- DOI: 10.1215/15228517-2008-076
Adult gliosarcoma: epidemiology, natural history, and factors associated with outcome
Abstract
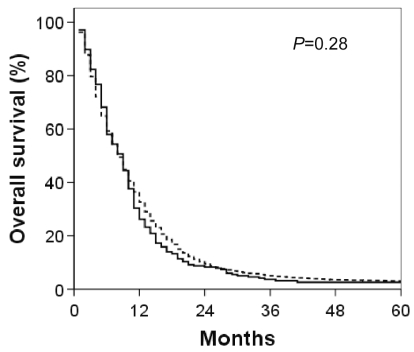
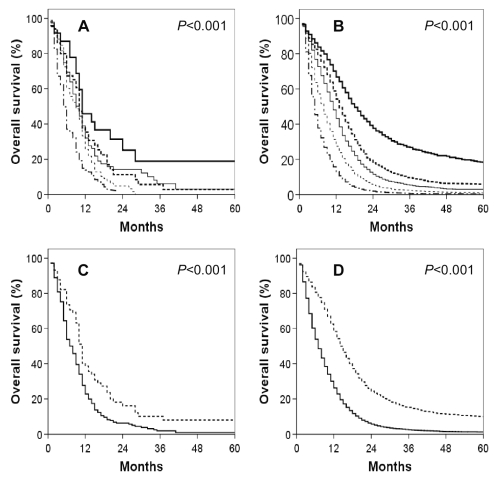
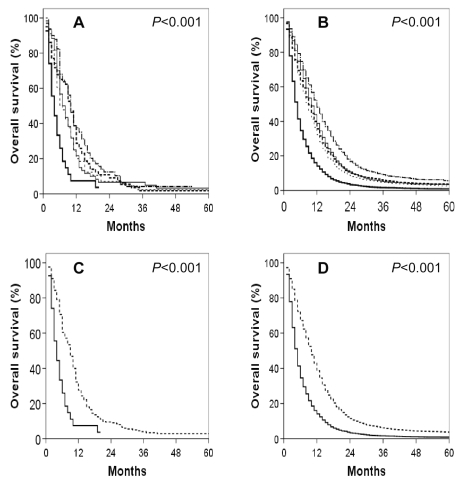
The epidemiology and natural history of adult gliosarcomas (GSMs), as well as patient and treatment factors associated with outcome, are ill defined. Patients over 20 years of age with GSM diagnosed from 1988 to 2004 were identified in the Surveillance, Epidemiology, and End Results (SEER) database. Kaplan-Meier survival analysis and Cox models were used to examine outcomes. Similar analyses were conducted for patients diagnosed with glioblastoma (GBM) over the same time period. GSM represented 2.2% of the 16,388 patients identified with either GSM or GBM. No significant differences between GSM and GBM were identified with respect to age, gender, race, tumor size, or use of adjuvant radiation therapy (RT). Patients with GSM were more likely to have temporal lobe involvement and undergo some form of tumor resection. The most important analyzed factors influencing GSM overall survival were age, extent of resection, and use of adjuvant RT. After adjusting for factors impacting overall survival, the prognosis for GSM appears slightly worse than for GBM (HR = 1.17, 95% CI, 1.05-1.31). GSM is a rare malignancy that presents very similarly to GBM with a slightly greater propensity for temporal lobe involvement. Optimal treatment remains to be defined. However, these retrospective findings suggest tumor excision, as opposed to biopsy only, and adjuvant RT may improve outcome. Despite therapy, prognosis remains dismal and outcomes may be inferior to those seen in GBM patients.
Figures

References
-
- Stroebe H. Uber Entstehung und Bau der Gehirngliome. Beitr Pathol Anat Allg Pathol. 1895;18:405–486.
-
- Meis JM, Martz KL, Nelson JS. Mixed glioblastoma multiforme and sarcoma. A clinicopathologic study of 26 Radiation Therapy Oncology Group cases. Cancer. 1991;67:2342–2349. - PubMed
-
- Morantz RA, Feigen I, Ransohoff J. Clinical and pathological study of 24 cases of gliosarcoma. J Neurosurg. 1976;45:398–408. - PubMed
-
- Salvati M, Caroli E, Raco A, Giangaspero F, Delfini R, Ferrante L. Gliosarcomas: Analysis of 11 cases do two subtypes exist? J Neurooncol. 2005;74:59–63. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
