

The Canadian Benign Prostatic Hyperplasia Audit Study (CanBas)
- PMID: 18781209
- PMCID: PMC2532544
- DOI: 10.5489/cuaj.629
The Canadian Benign Prostatic Hyperplasia Audit Study (CanBas)
Abstract
Objective: To determine the prevalence, diagnostic patterns and management of lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) in Canadian urology outpatient practice.
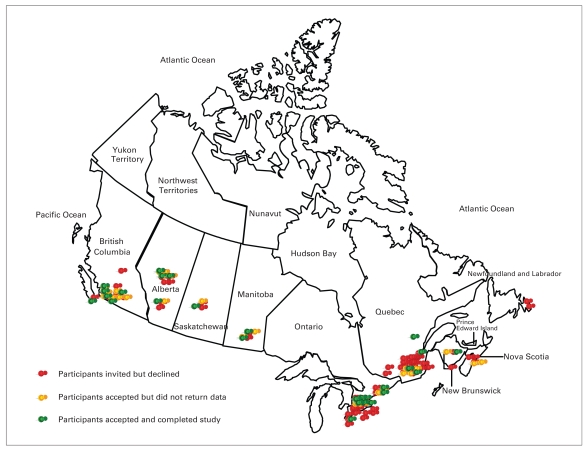
Methods: Representative urologists were randomly selected from lists provided by the Canadian and Quebec Urological Associations. Each patient identified with a BPH diagnosis during a typical 2-consecutive-week period during April, May or June 2007 was asked to complete a corresponding International Prostate Symptom Score (IPSS) questionnaire. Each day, the participant urologist completed an outpatient log and a detailed programmed chart review to transcribe demographics, investigations and treatments associated with each BPH patient.
Results: Eighty-six urologists were invited to participate. Thirty-eight (44.2%) agreed, and 27 of those (71.1%) submitted evaluable data for the audit. Of the 5616 patients seen in outpatient practice (average 208 per urologist), 4324 (77%) were male. A BPH diagnosis was identified in 19.6% of the men (n = 849; mean age 69.5, standard deviation [SD] 10, yr; age range 40-100 yr; mean duration of symptoms 4.8, SD 4.2, yr; mean IPSS score 12.3, SD 7.4; mean prostate specific antigen [PSA] 3.9, SD 3.9, ng/mL). Twenty-four percent of patients had prostates that were rated as large, 50% as medium and 26% as small. PSA level correlated positively with prostate volume. Twenty-two percent were initial consultations for LUTS and 78% were repeat visits. Diagnostic evaluation tended to follow those examinations and tests recommended by the Canadian BPH guidelines. Treatment choices tended to follow an evidence-based algorithm with respect to treatment choices for men in the various prostate-volume and PSA groups.
Conclusion: This prospective audit indicates that BPH remains a common condition managed by urologists in outpatient practice. Investigations and treatments confirm that Canadian urologists appear to be following Canadian BPH guidelines as well as the most recent evidence from the literature.
Figures
References
-
- Nickel JC, Herschorn S, Corcos J, et al. Canadian Guidelines for the Management of Benign Prostatic Hyperplasia. Can J Urol. 2005;12:2677–83. - PubMed
-
- Roehrborn CG, Siami P, Barkin J, et al. Effects of dutasteride, tamsulosin and combination therapy on lower urinary tract symptoms in men with benign prostatic hyperplasia and prostatic enlargement: 2-year results from CombAT study. J Urol. 2008;179:616–21. - PubMed
-
- Ramsey EW, Elhilali M, Goldenberg GS, et al. Canadian Prostate Health Council. Practice patterns of Canadian urologists in benign prostatic hyperplasia and prostate cancer. J Urol. 2000;163:499–502. - PubMed
-
- McConnell JD, Roehrborn CG, Oliver OM, et al. MTOPS Research Group. The long term effect of doxazosin, finasteride and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2385–96. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
