

Pediatric urolithiasis: experience at a tertiary care pediatric hospital
- PMID: 18781210
- PMCID: PMC2532545
- DOI: 10.5489/cuaj.804
Pediatric urolithiasis: experience at a tertiary care pediatric hospital
Abstract
Objective: We aimed to determine the epidemiology, risk factors, clinical characteristics, evaluation and course of patients with urolithiasis at the Children's Hospital of Eastern Ontario to improve current diagnostic and management strategies.
Methods: This was a retrospective study of children with newly identified urolithiasis between Jan. 1, 1999, and July 31, 2004. Cases were reviewed for demographics, presentation, family history, diagnostic methods and findings, metabolic and anatomic abnormalities, management, stone analysis and stone recurrence.
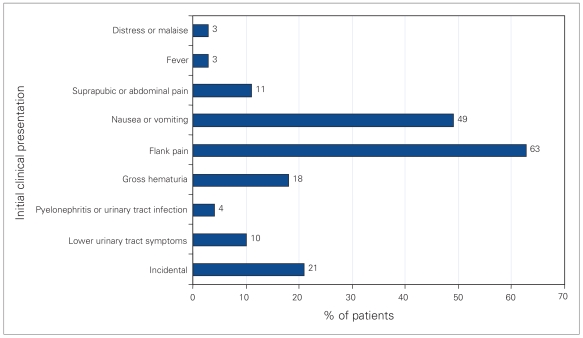
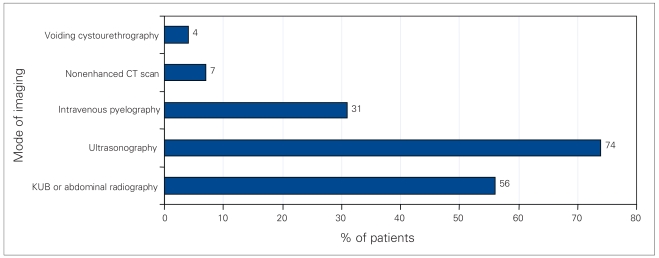
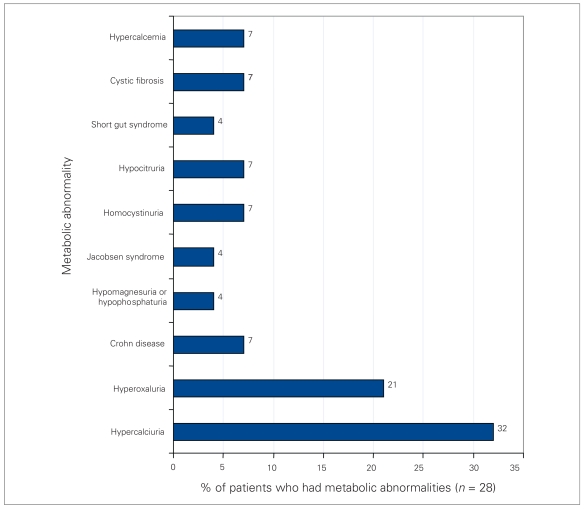
Results: Seventy-two patients (40 male, 32 female; mean age 11.3 yr) were assessed. Mean follow-up was at 1.5 years. Eighteen patients (25%) had a family history of stones. Flank pain (63%) was the most common presentation. Eighty-two percent of urinalyses showed microscopic hematuria. Imaging comprised abdominal plain film radiography (56%) and (or) abdominal ultrasonography (74%). The mean stone size was 5 mm. Forty-one percent (28/69) of patients who underwent metabolic investigation had an abnormality. Fourteen percent of patients (10/72) had a genitourinary anatomical abnormality. Thirty-four patients (47%) passed their stones spontaneously, 25 patients (35%) required surgical intervention and 13 patients (18%) had yet to pass their stone. The mean size of spontaneously passed stones was 4 mm. Of 42 stones analyzed, 39 (93%) were composed of calcium oxalate or phosphate. Seventeen (24%) patients had stone recurrence during follow-up.
Conclusion: Pediatric patients with stones present in a manner similar to adults. Abdominal plain film radiography and ultrasonography are the preferred initial radiological investigations in children as they limit radiation exposure. Metabolic abnormalities are common and may coexist with anatomic abnormalities, therefore investigations must rule these out. One-half of patients will pass their stones spontaneously. Recurrence rates are high and long-term follow-up is recommended.
Figures
Similar articles
-
Comprehensive analysis of pediatric urolithiasis in a tertiary care center and insights into demographics, risk factors, and management outcomes.J Pediatr Urol. 2025 Mar 13:S1477-5131(25)00144-5. doi: 10.1016/j.jpurol.2025.03.006. Online ahead of print. J Pediatr Urol. 2025. PMID: 40133120
-
Pediatric urolithiasis: experience from a tertiary referral center.J Pediatr Urol. 2013 Dec;9(6 Pt A):825-30. doi: 10.1016/j.jpurol.2012.11.003. Epub 2013 Jan 21. J Pediatr Urol. 2013. PMID: 23348148
-
Pediatric urolithiasis: an 8-year experience of single centre.Int Urol Nephrol. 2008;40(1):3-9. doi: 10.1007/s11255-007-9234-6. Epub 2007 Jul 5. Int Urol Nephrol. 2008. PMID: 17611811
-
Why we need a higher suspicion index of urolithiasis in children.J Pediatr Urol. 2017 Apr;13(2):164-171. doi: 10.1016/j.jpurol.2016.12.021. Epub 2017 Jan 29. J Pediatr Urol. 2017. PMID: 28185760 Review.
-
[Urinary calculi epidemiology in children].Rev Med Suisse Romande. 2004 Aug;124(8):433-7. Rev Med Suisse Romande. 2004. PMID: 15495464 Review. French.
Cited by
-
The establishment of a standard and real patient kidney stone library utilizing Fourier transform-infrared spectroscopy with a diamond ATR accessory.Urol Res. 2012 Oct;40(5):483-98. doi: 10.1007/s00240-011-0456-9. Epub 2012 Jan 13. Urol Res. 2012. PMID: 22246314
-
Epidemiology of pediatric urolithiasis.Indian J Urol. 2010 Oct;26(4):516-22. doi: 10.4103/0970-1591.74450. Indian J Urol. 2010. PMID: 21369384 Free PMC article.
-
The increasing pediatric stone disease problem.Ther Adv Urol. 2011 Feb;3(1):3-12. doi: 10.1177/1756287211400491. Ther Adv Urol. 2011. PMID: 21789094 Free PMC article.
-
Current medical treatment in pediatric urolithiasis.Turk J Urol. 2013 Dec;39(4):253-63. doi: 10.5152/tud.2013.063. Turk J Urol. 2013. PMID: 26328120 Free PMC article. Review.
-
Educational review: role of the pediatric nephrologists in the work-up and management of kidney stones.Pediatr Nephrol. 2020 Mar;35(3):383-397. doi: 10.1007/s00467-018-4179-9. Epub 2019 Jan 4. Pediatr Nephrol. 2020. PMID: 30607567 Review.
References
-
- Rizvi SAH, Naqvi SA, Hussain Z, et al. Pediatric urolithiasis: developing nations perspectives. J Urol. 2002;168:1522–5. - PubMed
-
- Marx JA, Hockberger S, Walls RM, et al., editors. Rosen’s emergency medicine: concepts and clinical practice. 5. St. Louis (MO): Mosby; 2002. p. 2234.
-
- Kroovand RL. Pediatric urolithiasis. Urol Clin North Am. 1997;24:173–84. - PubMed
-
- Erbagci A, Erbagci AB, Yilmaz M, et al. Pediatric urolithiasis. Scand J Urol Nephrol. 2002;37:129–33. - PubMed
-
- Milliner DS, Murphy ME. Urolithiasis in pediatric patients. Mayo Clin Proc. 1993;68:241–8. - PubMed
LinkOut - more resources
Full Text Sources
