

Birth injury of the cranium and central nervous system
- PMID: 18782168
- PMCID: PMC8095602
- DOI: 10.1111/j.1750-3639.2008.00205.x
Birth injury of the cranium and central nervous system
Abstract
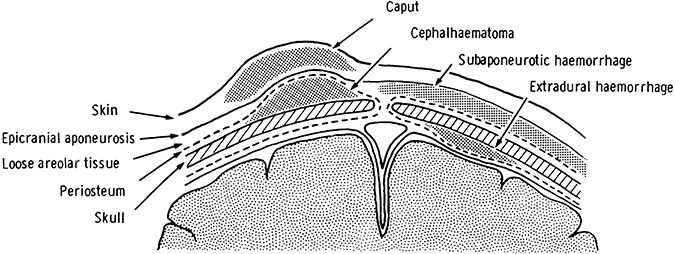
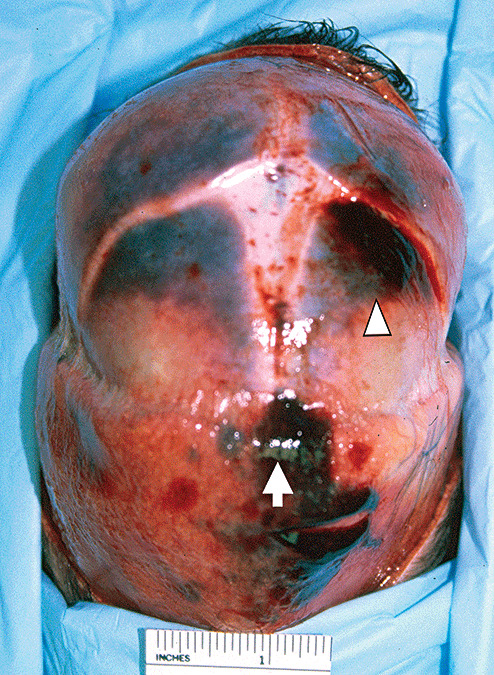
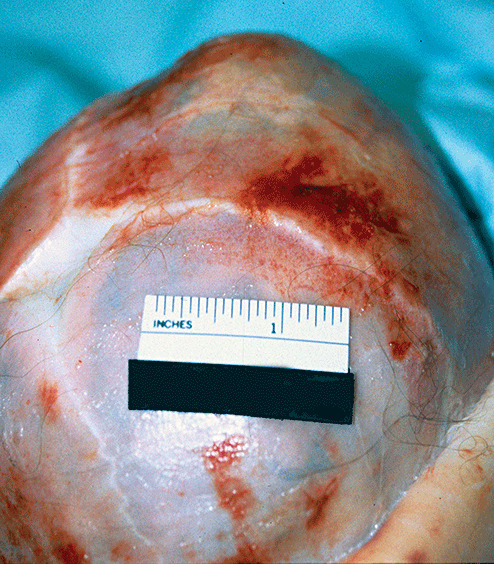
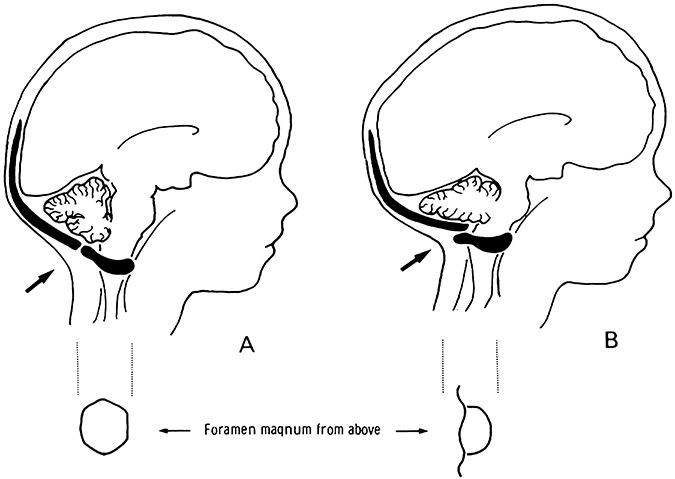
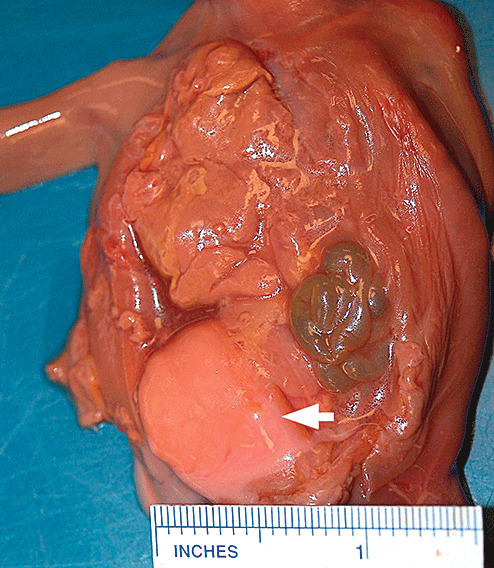
Birth injury of the scalp, skull and central nervous system (CNS) is a well-recognized complication of a difficult delivery. The rate of birth trauma has dropped precipitously and now accounts for less than 2% of neonatal deaths. Despite this dramatic decrease in birth-trauma mortality significant injuries still occur. A variety of risk factors clearly predispose certain infants to birth-related injury. Recent neuroradiology studies indicate that intracranial hemorrhage, even in asymptomatic infants, is not rare. Pathologists' (neuropathologists and forensic pathologists) appreciation of the spectrum of birth injuries and their sequelae is critical in order to be able to distinguish these from inflicted injuries and post-mortem changes.
Figures
References
-
- Bobinski L, Bostrom S, Zsigmond P, Theodorsson A (2007) Leptomeningeal cyst due to vacuum extraction delivery in a twin infant. Acta Neurochir (Wien) 149:319–323. - PubMed
-
- Chenoy R, Johanson R (1992) A randomized prospective study comparing delivery with metal and silicone rubber vacuum extractor cups. Br J Obstet Gynaecol 99:360–363. - PubMed
-
- Clement R, Bresson C, Marcorelles P, Rodat O, Lagarde N (2006) Cerebellar‐pulmonary embolism, cause of death in the newborn. J Clin Forensic Med 13:361–365. - PubMed
-
- Cumming WA (1979) Neonatal skeletal fractures. Birth trauma or child abuse? J Can Assoc Radiol 30:30–33. - PubMed
-
- Djientcheu VD, Rilliet B, Delavelle J, Argyropoulo M, Gudinchet F, De Tribolet N (1996) Leptomeningeal cyst in newborns due to vacuum extraction: report of two cases. Childs Nerv Syst 12: 399–403. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
