

Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer
- PMID: 18783876
- PMCID: PMC10651170
- DOI: 10.1016/j.eururo.2008.08.051
Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer
Abstract
Background: Nonrandomized studies of unilateral nerve-sparing (UNS) radical prostatectomy (RP) have reported improved recovery of erectile function if the sacrificed cavernous nerve is reconstructed with a sural nerve graft (SNG).
Objective: To determine whether UNS RP plus SNG results in a 50% relative increase in potency at 2 yr compared to UNS RP alone.
Design, setting, and participants: The study enrolled patients from October 2001-May 2006 from a single academic center and was randomized, open label. Participants were men with localized prostate cancer recommended for UNS RP, less than 66 yr old, normal baseline erectile function, and willing to participate in early erectile dysfunction (ED) therapy. Patients were followed up to 2 yr.
Intervention: Patients underwent UNS RP and ED therapy starting at 6 wk: oral prostaglandin type-5 (PDE5) inhibitor, vacuum erection device (VED), and intracavernosal injection therapy. In the SNG group, a plastic surgeon performed the procedure at the time of RP.
Measurements: The ability to have an erection suitable for intercourse with or without a PDE5 inhibitor at 2 yr. The hypothesis was that SNG would result in a 60% potency rate compared to 40% for controls (80% power, 5% two-way significance).
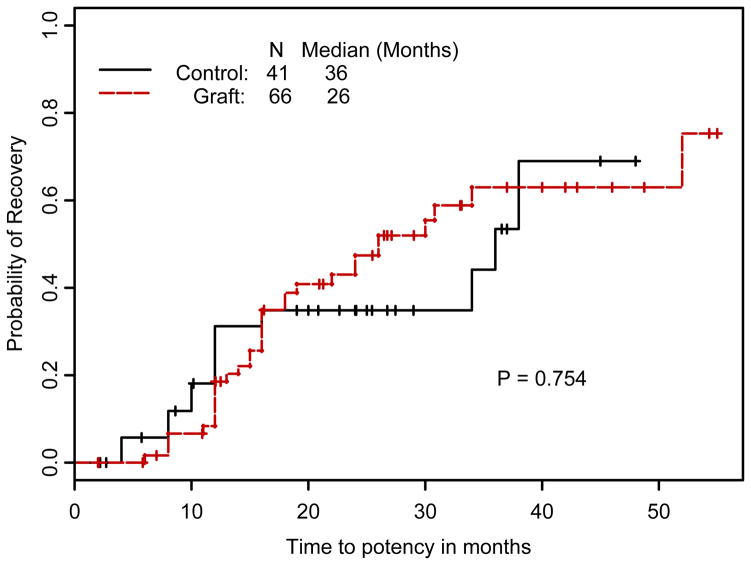
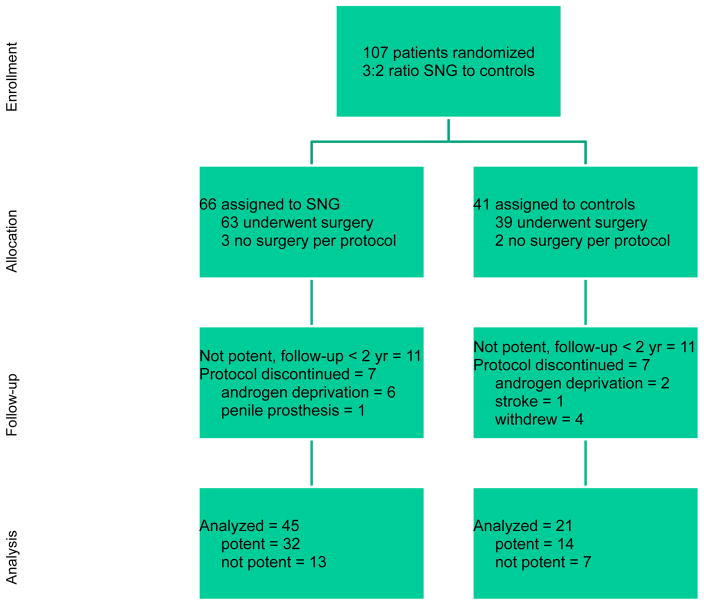
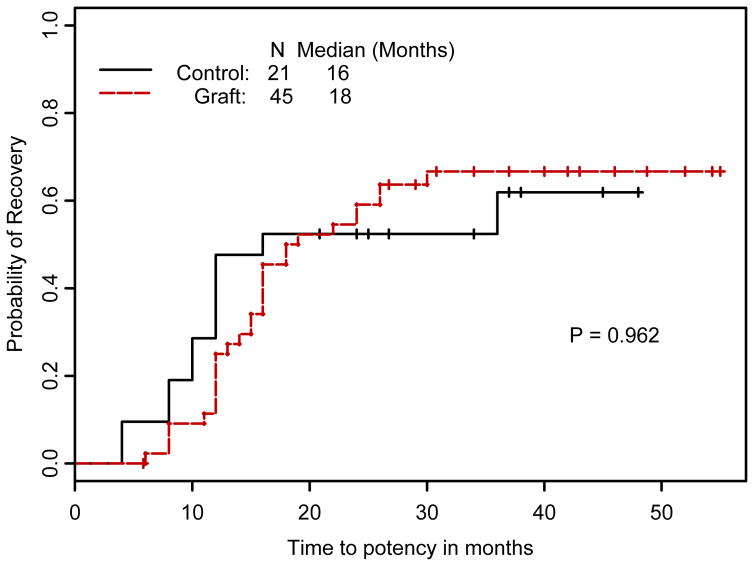
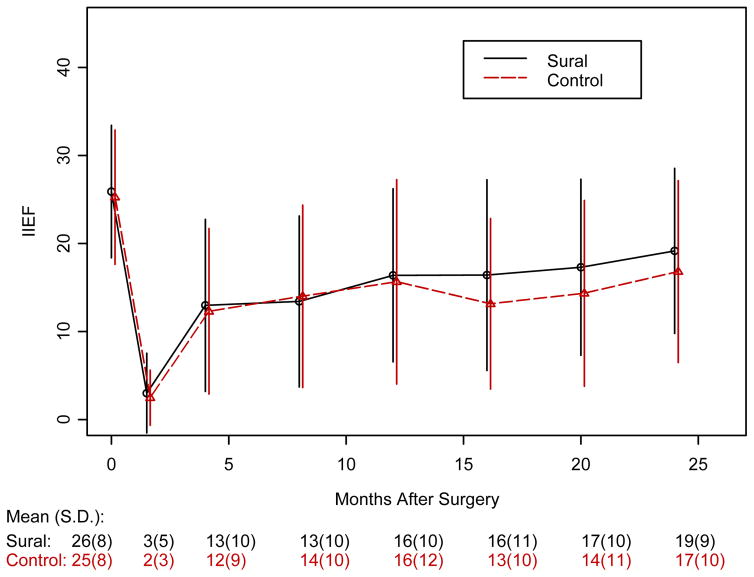
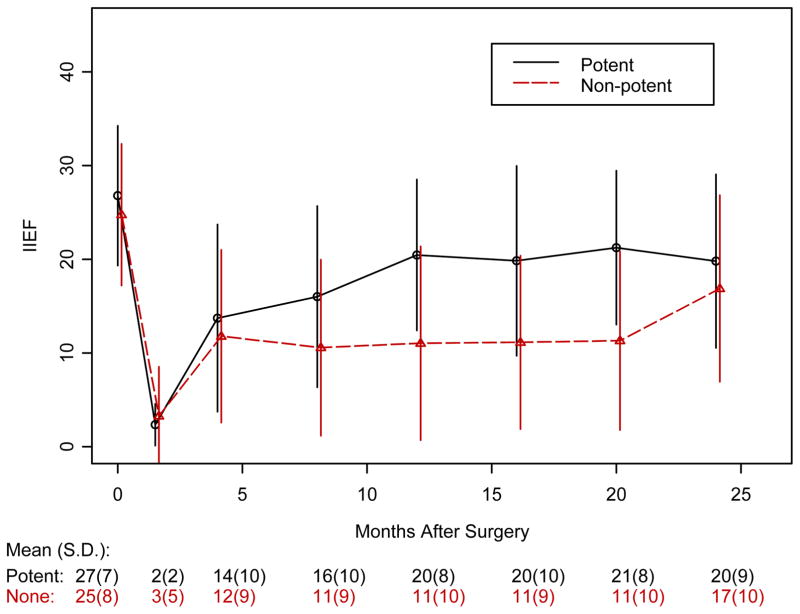
Results and limitations: The trial planned to enroll 200 patients, but an interim analysis at 107 patients met criteria for futility and the trial was closed. For patients completing the protocol to 2 yr, potency was recovered in 32 of 45 (71%) of SNG and 14 of 21 (67%) of controls (p=0.777). By intent-to-treat analysis, potency recovered in 32 of 66 (48.5%) of SNG and 14 of 41 (34%) of controls (p=0.271). No differences were seen in time to potency or quality of life scores for ED and urinary function. Limitations included slower-than-expected accrual and poor compliance with ED therapy: <65% for VED and <40% for injections.
Conclusions: The addition of SNG to a UNS RP did not improve potency at 2 yr following surgery.
Trial registration: ClinicalTrials.gov, Identifier: NCT00080808, http://www.clinicaltrials.gov/ct2/show/NCT00080808?term=NCT00080808&rank=1.
Figures
Comment in
-
Editorial comment on: Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer.Eur Urol. 2009 May;55(5):1143. doi: 10.1016/j.eururo.2008.08.052. Epub 2008 Sep 2. Eur Urol. 2009. PMID: 18783871 Clinical Trial. No abstract available.
-
Editorial comment on: Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer.Eur Urol. 2009 May;55(5):1144. doi: 10.1016/j.eururo.2008.08.053. Epub 2008 Sep 2. Eur Urol. 2009. PMID: 18783874 Clinical Trial. No abstract available.
Similar articles
-
Editorial comment on: Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer.Eur Urol. 2009 May;55(5):1143. doi: 10.1016/j.eururo.2008.08.052. Epub 2008 Sep 2. Eur Urol. 2009. PMID: 18783871 Clinical Trial. No abstract available.
-
Editorial comment on: Randomized phase II trial evaluation of erectile function after attempted unilateral cavernous nerve-sparing retropubic radical prostatectomy with versus without unilateral sural nerve grafting for clinically localized prostate cancer.Eur Urol. 2009 May;55(5):1144. doi: 10.1016/j.eururo.2008.08.053. Epub 2008 Sep 2. Eur Urol. 2009. PMID: 18783874 Clinical Trial. No abstract available.
-
Three-year outcomes of recovery of erectile function after open radical prostatectomy with sural nerve grafting.J Sex Med. 2014 Aug;11(8):2119-24. doi: 10.1111/jsm.12600. Epub 2014 Jun 5. J Sex Med. 2014. PMID: 24903070
-
Strategies to promote recovery of cavernous nerve function after radical prostatectomy.World J Urol. 2003 May;20(6):337-42. doi: 10.1007/s00345-002-0303-2. Epub 2002 Dec 10. World J Urol. 2003. PMID: 12811492 Review.
-
[Prevention and treatment of erectile dysfunction after prostatectomy: An update].Zhonghua Nan Ke Xue. 2017 Jul;23(7):656-662. Zhonghua Nan Ke Xue. 2017. PMID: 29723462 Review. Chinese.
Cited by
-
Evolution in the concept of erection anatomy.Surg Radiol Anat. 2011 May;33(4):301-12. doi: 10.1007/s00276-010-0707-4. Epub 2010 Aug 5. Surg Radiol Anat. 2011. PMID: 20686767 Review.
-
Inside-out autologous vein grafts fail to restore erectile function in a rat model of cavernous nerve crush injury after nerve-sparing prostatectomy.Int J Impot Res. 2015 Mar-Apr;27(2):59-62. doi: 10.1038/ijir.2014.32. Epub 2014 Jul 31. Int J Impot Res. 2015. PMID: 25078050
-
Emerging tools for erectile dysfunction: a role for regenerative medicine.Nat Rev Urol. 2012 Sep;9(9):520-36. doi: 10.1038/nrurol.2012.143. Epub 2012 Jul 24. Nat Rev Urol. 2012. PMID: 22824778 Review.
-
Erectile dysfunction following prostatectomy: prevention and treatment.Nat Rev Urol. 2009 Aug;6(8):415-27. doi: 10.1038/nrurol.2009.126. Nat Rev Urol. 2009. PMID: 19657376 Review.
-
Decade in review-sexual dysfunction: post-RP erectile dysfunction-therapies for the next decade.Nat Rev Urol. 2014 Nov;11(11):616-8. doi: 10.1038/nrurol.2014.274. Epub 2014 Sep 30. Nat Rev Urol. 2014. PMID: 25266570 No abstract available.
References
-
- Kim ED, Scardino PT, Hampel O, et al. Interposition of sural nerve restores function of cavernous nerves resected during radical prostatectomy. J Urol. 1999;161:188. [en]92. - PubMed
-
- Kim ED, Nath R, Slawin KM, et al. Bilateral nerve grafting during radical retropubic prostatectomy: extended follow-up. Urology. 2001;58:983. [en]7. - PubMed
-
- Chang DW, Wood CG, Kroll SS, et al. Cavernous nerve reconstruction to preserve erectile function following non-nerve-sparing radical retropubic prostatectomy: a prospective study. Plast Reconstr Surg. 2003;111:1174. [en]81. - PubMed
-
- Galper SL, Chen MH, Catalona WJ, et al. Evidence to support a continued stage migration and decrease in prostate cancer specific mortality. J Urol. 2006;175:907. [en]12. - PubMed
-
- Sokoloff MH, Brendler CB. Indications and contraindications for nerve-sparing radical prostatectomy. Urol Clin North Am. 2001;28:535. [en]43. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
