

Early mortality among adults accessing antiretroviral treatment programmes in sub-Saharan Africa
- PMID: 18784453
- PMCID: PMC3816249
- DOI: 10.1097/QAD.0b013e32830007cd
Early mortality among adults accessing antiretroviral treatment programmes in sub-Saharan Africa
Abstract
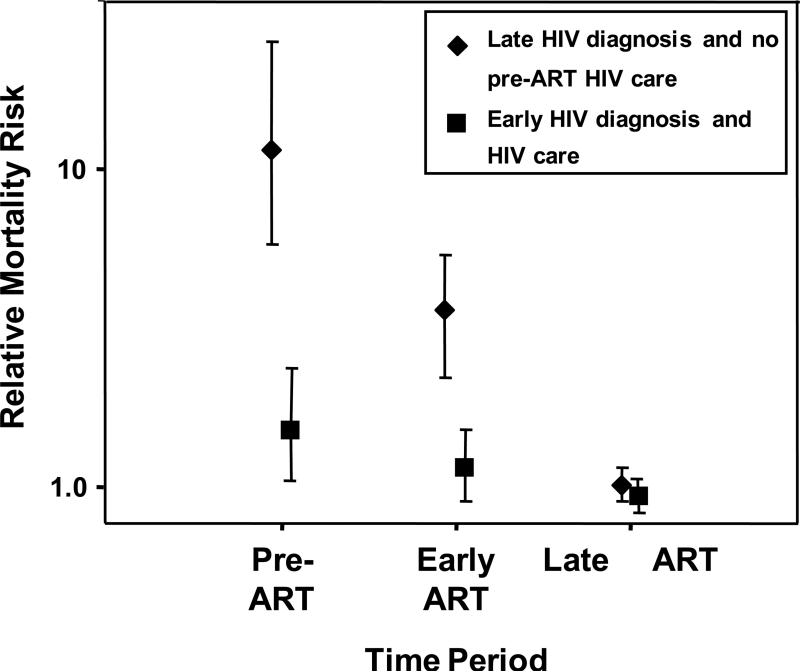
Two-thirds of the world's HIV-infected people live in sub-Saharan Africa, and more than 1.5 million of them die annually. As access to antiretroviral treatment has expanded within the region; early pessimism concerning the delivery of antiretroviral treatment using a large-scale public health approach has, at least in the short term, proved to be broadly unfounded. Immunological and virological responses to ART are similar to responses in patients treated in high-income countries. Despite this, however, early mortality rates in sub-Saharan Africa are very high; between 8 and 26% of patients die in the first year of antiretroviral treatment, with most deaths occurring in the first few months. Patients typically access antiretroviral treatment with advanced symptomatic disease, and mortality is strongly associated with baseline CD4 cell count less than 50 cells/mul and WHO stage 4 disease (AIDS). Although data are limited, leading causes of death appear to be tuberculosis, acute sepsis, cryptococcal meningitis, malignancy and wasting syndrome. Mortality rates are likely to depend not only on the care delivered by antiretroviral treatment programmes, but more fundamentally on how advanced disease is at programme enrollment and the quality of preceding healthcare. In addition to improving delivery of antiretroviral treatment and providing it free of charge to the patient, strategies to reduce mortality must include earlier diagnosis of HIV infection, strengthening of longitudinal HIV care and timely initiation of antiretroviral treatment. Health systems delays in antiretroviral treatment initiation must be minimized, especially in patients who present with advanced immunodeficiency.
Figures

References
-
- Palella FJ, Jr., Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Egger M, May M, Chene G, Phillips AN, Ledergerber B, Dabis F, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–129. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, Kirk O, Reiss P, d'Arminio MA, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet. 2003;362:22–29. - PubMed
-
- UNAIDS / WHO AIDS epidemic update 2007. http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf.
-
- World Health Organization . Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report, April 2007. WHO; Geneva: 2007. [24.04.07]. http://www.who.int/hiv/toronto2006/towardsuniversalaccess.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
