

Use of T2-weighted magnetic resonance imaging of the optic nerve sheath to detect raised intracranial pressure
- PMID: 18786243
- PMCID: PMC2592740
- DOI: 10.1186/cc7006
Use of T2-weighted magnetic resonance imaging of the optic nerve sheath to detect raised intracranial pressure
Abstract
Introduction: The dural sheath surrounding the optic nerve communicates with the subarachnoid space, and distends when intracranial pressure is elevated. Magnetic resonance imaging (MRI) is often performed in patients at risk for raised intracranial pressure (ICP) and can be used to measure precisely the diameter of optic nerve and its sheath. The objective of this study was to assess the relationship between optic nerve sheath diameter (ONSD), as measured using MRI, and ICP.
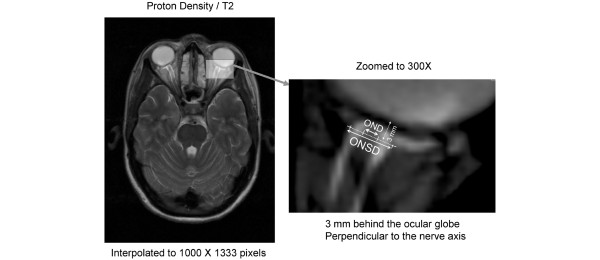
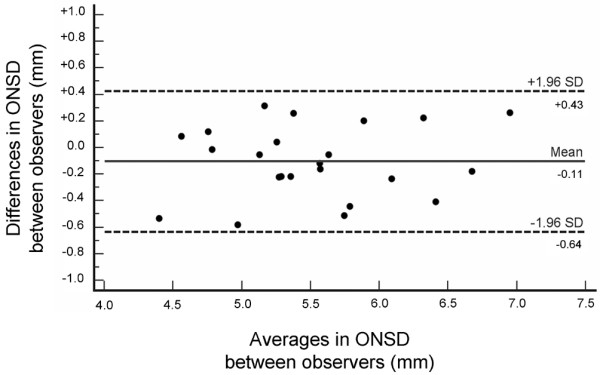
Methods: We conducted a retrospective blinded analysis of brain MRI images in a prospective cohort of 38 patients requiring ICP monitoring after severe traumatic brain injury (TBI), and in 36 healthy volunteers. ONSD was measured on T2-weighted turbo spin-echo fat-suppressed sequence obtained at 3 Tesla MRI. ICP was measured invasively during the MRI scan via a parenchymal sensor in the TBI patients.
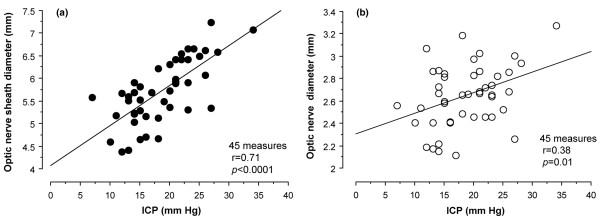
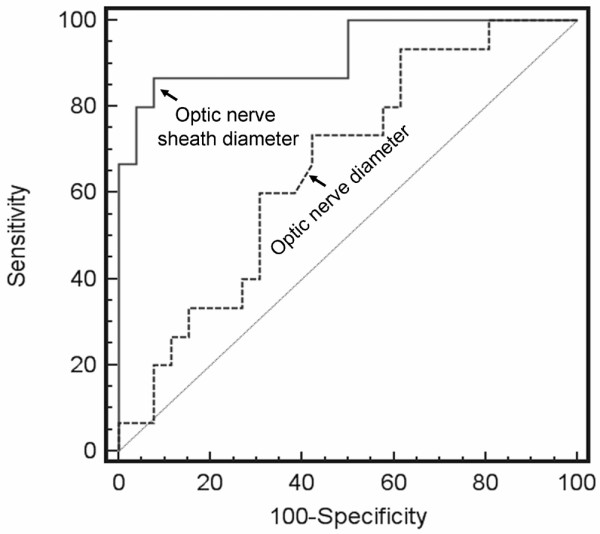
Results: Measurement of ONSD was possible in 95% of cases. The ONSD was significantly greater in TBI patients with raised ICP (>20 mmHg; 6.31 +/- 0.50 mm, 19 measures) than in those with ICP of 20 mmHg or less (5.29 +/- 0.48 mm, 26 measures; P < 0.0001) or in healthy volunteers (5.08 +/- 0.52 mm; P < 0.0001). There was a significant relationship between ONSD and ICP (r = 0.71, P < 0.0001). Enlarged ONSD was a robust predictor of raised ICP (area under the receiver operating characteristic curve = 0.94), with a best cut-off of 5.82 mm, corresponding to a negative predictive value of 92%, and to a value of 100% when ONSD was less than 5.30 mm.
Conclusions: When brain MRI is indicated, ONSD measurement on images obtained using routine sequences can provide a quantitative estimate of the likelihood of significant intracranial hypertension.
Figures
Comment in
-
Using MRI of the optic nerve sheath to detect elevated intracranial pressure.Crit Care. 2008;12(5):181. doi: 10.1186/cc7008. Epub 2008 Sep 24. Crit Care. 2008. PMID: 18831721 Free PMC article.
References
-
- Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, Amelink GJ, Schmiedeck P, Schwab S, Rothwell PM, Bousser MG, Worp HB van der, Hacke W, DECIMAL, DESTINY, and HAMLET investigators Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol. 2007;6:215–222. doi: 10.1016/S1474-4422(07)70036-4. - DOI - PubMed
-
- Ware AJ, D'Agostino AN, Combes B. Cerebral edema: a major complication of massive hepatic necrosis. Gastroenterology. 1971;61:877–884. - PubMed
-
- Quagliarello V, Scheld WM. Bacterial meningitis: pathogenesis, pathophysiology, and progress. N Engl J Med. 1992;327:864–872. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
