

The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee
- PMID: 18786841
- PMCID: PMC3048821
- DOI: 10.1016/j.joca.2008.06.016
The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee
Abstract
Objectives: To report on the process and criteria for selecting acquisition protocols to include in the osteoarthritis initiative (OAI) magnetic resonance imaging (MRI) study protocol for the knee.
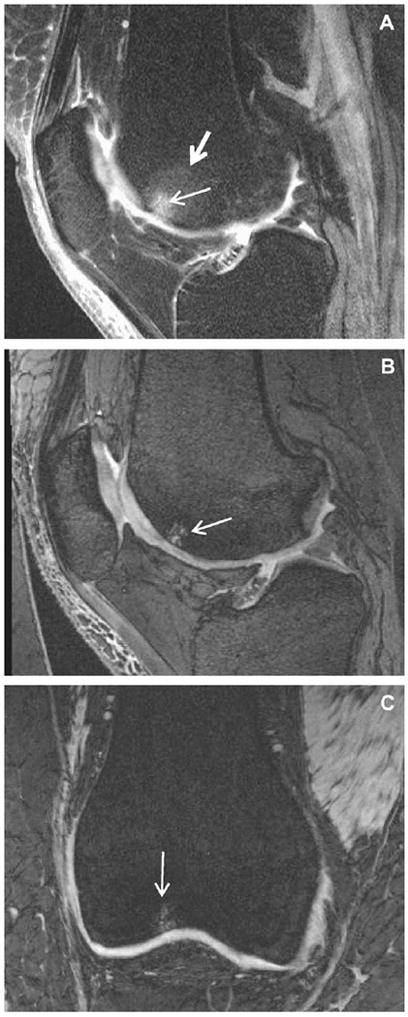
Methods: Candidate knee MR acquisition protocols identified from the literature were first optimized at 3Tesla (T). Twelve knees from 10 subjects were scanned one time with each of 16 acquisitions considered most likely to achieve the study goals and having the best optimization results. The resultant images and multi-planar reformats were evaluated for artifacts and structural discrimination of articular cartilage at the cartilage-fluid, cartilage-fat, cartilage-capsule, cartilage-meniscus and cartilage-cartilage interfaces.
Results: The five acquisitions comprising the final OAI MRI protocol were assembled based on the study goals for the imaging protocol, the image evaluation results and the need to image both knees within a 75 min time slot, including positioning. For quantitative cartilage morphometry, fat-suppressed, 3D dual-echo in steady state (DESS) acquisitions appear to provide the best universal cartilage discrimination.
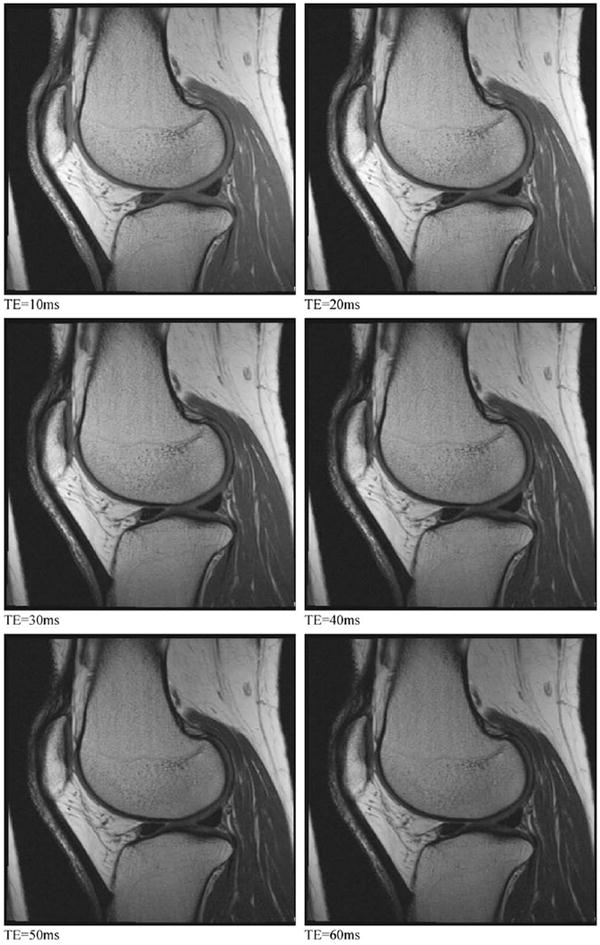
Conclusions: The OAI knee MRI protocol provides imaging data on multiple articular structures and features relevant to knee OA that will support a broad range of existing and anticipated measurement methods while balancing requirements for high image quality and consistency against the practical considerations of a large multi-center cohort study. Strengths of the final knee MRI protocol include cartilage quantification capabilities in three planes due to multi-planar reconstruction of a thin slice, high spatial resolution 3D DESS acquisition and the multiple, non-fat-suppressed image contrasts measured during the T2 relaxation time mapping acquisition.
Conflict of interest statement
Figures



References
-
- Peterfy CG, Gold G, Eckstein F, Cicuttini F, Dardzinski B, Stevens R. MRI protocols for whole-organ assessment of the knee in osteoarthritis. Osteoarthritis Cartilage. 2006;14(Suppl A):A95–A111. - PubMed
-
- Gold GE, Burstein D, Dardzinski B, Lang P, Boada F, Mosher T. MRI of articular cartilage in OA: novel pulse sequences and compositional/-functional markers. Osteoarthritis Cartilage. 2006;14(Suppl A):A76–86. - PubMed
-
- Eckstein F, Cicuttini F, Raynauld JP, Waterton JC, Peterfy C. Magnetic resonance imaging (MRI) of articular cartilage in knee osteoarthritis (OA): morphological assessment. Osteoarthritis Cartilage. 2006;14(Suppl A):A46–75. - PubMed
-
- Eckstein F, Mosher T, Hunter D. Imaging of knee osteoarthritis: data beyond the beauty. Curr Opin Rheumatol. 2007;19(5):435–43. - PubMed
-
- Burstein D, Gray ML. Is MRI fulfilling its promise for molecular imaging of cartilage in arthritis? Osteoarthritis Cartilage. 2006;14(11):1087–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
