

Comparison of the 13C-urea breath test and the endoscopic phenol red mucosal pH test in the quantification of Helicobacter pylori infection loading
- PMID: 18787366
- PMCID: PMC2686969
- DOI: 10.3904/kjim.2008.23.3.134
Comparison of the 13C-urea breath test and the endoscopic phenol red mucosal pH test in the quantification of Helicobacter pylori infection loading
Abstract
Background/aims: The (13)C-urea breath test (UBT) is a semiquantitative test for measuring Helicobacter pylori infection loading. H. pylori produces ammonia, which elevates the pH of the gastric mucosa and is detectable via endoscopy using a phenol red indicator. We evaluated whether this test could be used to diagnose H. pylori infection and whether phenol red staining was correlated with (13)C-UBT results.
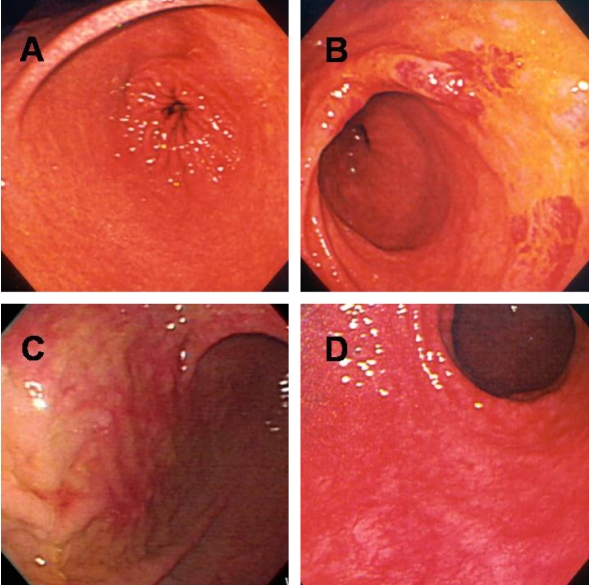
Methods: One hundred and twenty-three patients participated. The UBT was performed after ingestion of a capsule containing urea. A change in (13)C-UBT >2 ppt was selected as the cutoff value for diagnosing infection. After spraying evenly with a 0.1% phenol red solution, the pH of the gastric mucosal surface was measured using an antimony electrode through the biopsy channel.
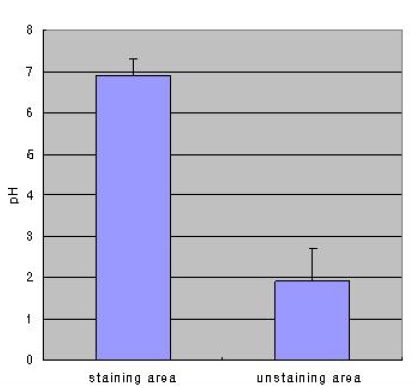
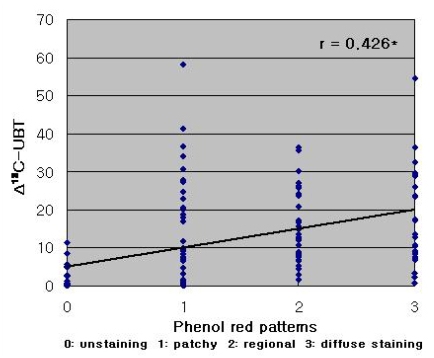
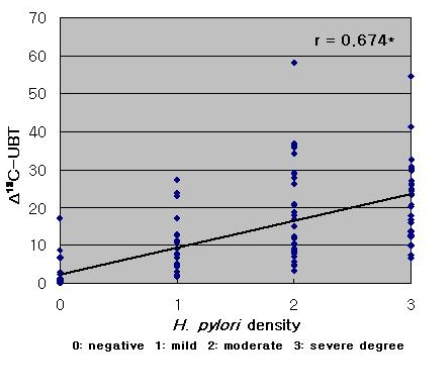
Results: The pH of stained mucosa (6.9+/-0.4) was significantly higher than that of unstained mucosa (1.9+/-0.8; p<0.001), and the H. pylori detection rate confirmed via histology was higher in stained versus unstained mucosa (p<0.01). Extensive mucosal staining resulted in a higher detection rate (p<0.001). The UBT produced results were very similar to those obtained via histological detection in stained mucosa (p<0.001). The extent of staining, expressed as a staining score, was positively correlated with the change in (13)C-UBT (r=0.426, p<0.001). A significant correlation was also observed between the histologically determined H. pylori density and (13)C-UBT results (r=0.674, p<0.001).
Conclusions: H. pylori infection elevates gastric mucosal surface pH, and endoscopic phenol red staining may be an alternative method for the diagnosis of H. pylori infection.
Conflict of interest statement
This study has not been previously published or submitted for publication elsewhere. The authors have no conflict of interest to declare.
Figures
References
-
- Warren JR, Marshall BJ. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet. 1983;1:1273–1275. - PubMed
-
- Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG. Helicobacter pylori-associated gastritis and primary B-cell gastric lymphoma. Lancet. 1991;338:1175–1176. - PubMed
-
- Parsonnet J, Friedman GD, Vandersteen DP, Chang Y, Vogelman JH, Orentreich N, Sibley RK. Helicobacter pylori infection and the riskof gastric carcinoma. N Engl J Med. 1991;325:1127–1131. - PubMed
-
- Basset C, Holton J, Ricci C, Gatta L, Tampieri A, Perna F, Miglioli M, Vaira D. Review article: diagnosis and treatment of Helicobacter: a 2002 updated review. Aliment Pharmacol Ther. 2003;17(Suppl 2):89–97. - PubMed
-
- Graham DY, Klein PD. Accurate diagnosis of Helicobacter pylori: 13C-urea breath test. Gastroenterol Clin North Am. 2000;29:885–893. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical