

The association between panic disorder and coronary artery disease among primary care patients presenting with chest pain: an updated literature review
- PMID: 18787675
- PMCID: PMC2528236
- DOI: 10.4088/pcc.v10n0402
The association between panic disorder and coronary artery disease among primary care patients presenting with chest pain: an updated literature review
Abstract
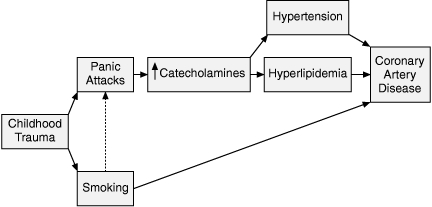
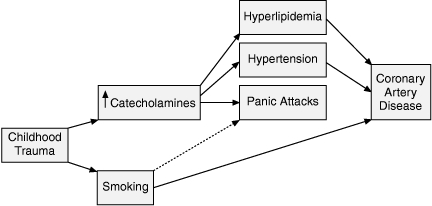
Context: Although panic disorder is linked to hypertension and smoking, the relationship between panic disorder and coronary artery disease (CAD) is unclear.
Objective: To extend our understanding about the strength of the association between panic disorder and coronary artery disease and known cardiovascular risk factors.
Data sources: Potential studies were identified via a computerized search of MEDLINE and PsycINFO databases and review of bibliographies. MeSH headings used included panic disorder with chest pain, panic disorder with coronary disease or cardiovascular disorders or heart disorders, and panic disorder with cholesterol or essential hypertension or tobacco smoking.
Study selection: The diagnosis of panic disorder in eligible studies was based on DSM-IV criteria, and studies must have used objective criteria for CAD and risk factors. Only case-control and cohort studies were included.
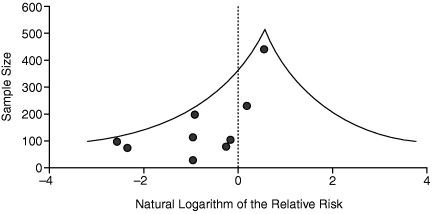
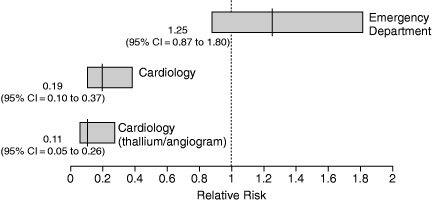
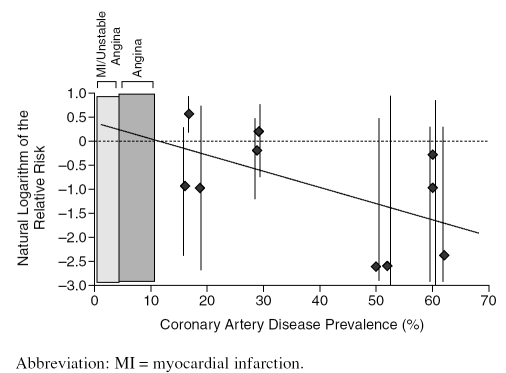
Data synthesis: Concerning the relationship between panic disorder and CAD, studies conducted in emergency departments found a relative risk [RR] of 1.25 (95% CI = 0.87 to 1.80), while those conducted in cardiology settings found an inverse relationship (RR = 0.19, 95% CI = 0.10 to 0.37). However, there is an inverse relationship between the prevalence of CAD in the study and the RR (r = -.554, p = .097), suggesting that, in primary care settings in which the prevalence of CAD is low, there may be a significant association between panic disorder and CAD.
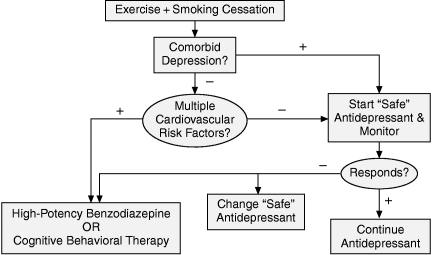
Conclusion: The association between panic disorder and CAD has several implications for primary care physicians managing patients with chest pain. When comorbid, the panic attacks may cause the patient with coronary disease to seek care but could also provoke a cardiac event. If one condition is recognized, a search for the other may be warranted because of the potential consequences if left undetected. The treatment approach to the panic disorder should be adjusted in the presence of comorbid CAD.
Figures
References
-
- Taylor CB, King R, and Ehlers A. et al. Treadmill exercise test and ambulatory measures in panic attacks. Am J Cardiol. 1987 60:48J–52J. - PubMed
-
- Goldberg R, Morris P, and Christian F. et al. Panic disorder in cardiac out-patients. Psychosomatics. 1990 31:168–173. - PubMed
-
- Kahn JP, Gorman JM, and King DL. et al. Cardiac left ventricular hypertrophy and chamber dilatation in panic disorder patients: implications for idiopathic dilated cardiomyopathy. Psychiatry Res. April1990 32(1):55–61. - PubMed
-
- Schmidt NB, Lerew DR, and Santiago H. et al. Effects of heart-rate feedback on estimated cardiovascular fitness in patients with panic disorder. Depress Anxiety. 2000 12:59–66. - PubMed
-
- Vural M, Akbas B, and Acer M. et al. Blood B-type natriuretic peptide level increases in patients who complain shortness of breath and chest pain in the course of panic attack. Int J Cardiol. April2007 117(2):e82–e83. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous