

Acute and chronic effects of continuous positive airway pressure therapy on left ventricular systolic and diastolic function in patients with obstructive sleep apnea and congestive heart failure
- PMID: 18787720
- PMCID: PMC2643175
- DOI: 10.1016/s0828-282x(08)70668-8
Acute and chronic effects of continuous positive airway pressure therapy on left ventricular systolic and diastolic function in patients with obstructive sleep apnea and congestive heart failure
Abstract
Background: Obstructive sleep apnea (OSA) may contribute to the pathogenesis of congestive heart failure (CHF). Nocturnal continuous positive airway pressure (CPAP) therapy can alleviate OSA and may have a role in the treatment of CHF patients.
Objectives: To investigate the acute and chronic effects of CPAP therapy on left ventricular systolic function, diastolic function and filling pressures in CHF patients with OSA.
Methods: Twelve patients with stable CHF (New York Heart Association II or III, radionuclide ejection fraction lower than 40%) underwent overnight polysomnography to detect OSA. In patients with OSA (n=7), echocardiography was performed at baseline (awake, before and during acute CPAP administration) and after 6.9+/-3.3 weeks of nocturnal CPAP therapy. Patients without OSA (n=5) did not receive CPAP therapy, but underwent a baseline and follow-up echocardiogram.
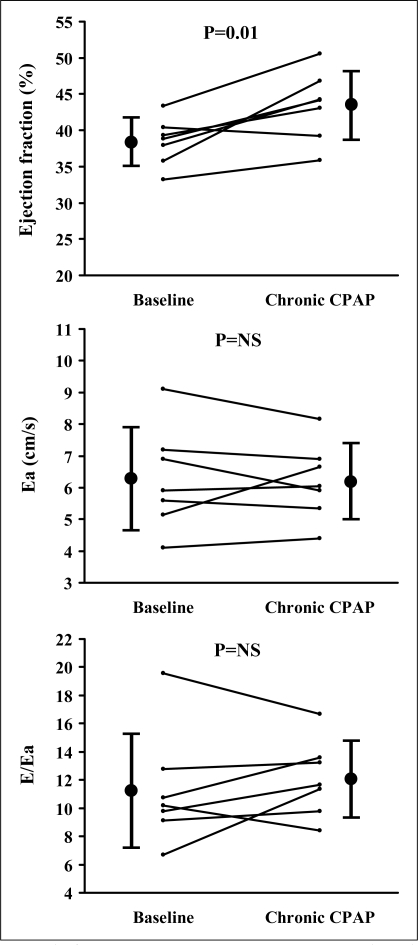
Results: In CHF patients with OSA, acute CPAP administration resulted in a decrease in stroke volume (44+/-15 mL versus 50+/-14 mL, P=0.002) and left ventricular ejection fraction ([LVEF] 34.8+/-5.0% versus 38.4+/-3.3%, P=0.006) compared with baseline, but no change in diastolic function or filling pressures (peak early diastolic mitral annular velocity [Ea]: 6.0+/-1.6 cm/s versus 6.3+/-1.6 cm/s, P not significant; peak early filling velocity to peak late filling velocity [E/A] ratio: 1.05+/-0.74 versus 1.00+/-0.67, P not significant; E/Ea ratio: 10.9+/-4.1 versus 11.3+/-4.1, P not significant). In contrast, chronic CPAP therapy resulted in a trend to an increase in stroke volume (59+/-19 mL versus 50+/-14 mL, P=0.07) and a significant increase in LVEF (43.4+/-4.8% versus 38.4+/-3.3%, P=0.01) compared with baseline, but no change in diastolic function or filling pressures (Ea: 6.2+/-1.2 cm/s versus 6.3+/-1.6 cm/s, P not significant; E/A ratio: 1.13+/-0.61 versus 1.00+/-0.67, P not significant; E/Ea ratio: 12.1+/-2.7 versus 11.3+/-4.1, P not significant). There was no change in left ventricular systolic function, diastolic function or filling pressures at follow-up in CHF patients without OSA.
Conclusions: Acute CPAP administration decreased stroke volume and LVEF in stable CHF patients with OSA. In contrast, chronic CPAP therapy for seven weeks improved left ventricular systolic function, but did not affect diastolic function or filling pressures. The potential clinical implications of the discrepant effects of CPAP therapy on left ventricular systolic and diastolic function in CHF patients with OSA warrant further study.
HISTORIQUE :: L’apnée obstructive du sommeil (AOS) peut contribuer à la pathogenèse de l’insuffisance cardiaque congestive (ICC). La thérapie nocturne par ventilation spontanée en pression positive continue (VSPPC) peut soulager l’AOS et pourrait être utile dans le traitement des patients atteints d’ICC.
OBJECTIFS :: Explorer les effets aigus et chroniques de la thérapie par VSPPC sur la fonction systolique, la fonction diastolique et les pressions de remplissage du ventricule gauche chez les patients atteints d’ICC présentant une AOS.
MÉTHODOLOGIE :: Douze patients atteints d’une ICC stable (stade III ou II de la New York Heart Association, fraction d’éjection par radionucléides inférieure à 40 %) ont subi une polysomnographie d’une nuit pour déceler l’AOS. Chez les patients présentant une AOS (n=7), les chercheurs ont procédé à une échocardiographie en début d’étude (en état d’éveil, avant et pendant l’administration aiguë de VSPPC) et après 6,9±3,3 semaines de thérapie nocturne par VSPPC. Les patients sans AOS (n=5) n’ont pas reçu de thérapie par VSPPC, mais ont subi un échocardiogramme en début d’étude et au moment du suivi.
RÉSULTATS :: Chez les patients présentant une AOS, l’administration aiguë de VSPPC a favorisé la diminution du volume d’accidents vasculaires cérébraux (AVC, soit 44±15 mL par rapport à 50±14 mL, P=0,002) et de la fraction d’éjection ventriculaire gauche (FÉVG, soit 34,8±5,0 % par rapport à 38,4±3,3 %, P=0,006) par rapport aux données de départ, mais aucun changement de la fonction diastolique ou des pressions de remplissage (vélocité protodiastolique de pointe de l’anneau mitral [Ea] : 6,0±1,6 cm/s par rapport à 6,3±1,6 cm/s, P non significatif; ratio entre la vélocité de remplissage précoce et la vélocité de remplissage tardive [E/A] : 1,05±0,74 par rapport à 1,00±0,67, P non significatif; ratio E/Ea : 10,9±4,1 par rapport à 11,3±4,1, P non significatif). Par contre, la thérapie chronique par VSPPC a provoqué une tendance à l’augmentation des AVC (59±19 mL par rapport à 50±14 mL, P=0,07) et une augmentation importante de la FÉVG (43,4±4,8 % par rapport 38,4±3,3 %, P=0,01) par rapport aux données de base, mais aucun changement de la fonction diastolique ou des pressions de remplissage (Ea : 6,2±1,2 cm/s par rapport à 6,3±1,6 cm/s, P non significatif; ratio E/A : 1,13±0,61 par rapport à 1,00±0,67, P non significatif; ratio E/Ea : 12,1±2,7 par rapport à 11,3±4,1, P non significatif). La fonction systolique ventriculaire gauche, la fonction diastolique et les pressions de remplissage n’avaient pas changé au suivi chez les patients atteints d’ICC sans AOS.
CONCLUSIONS :: L’administration aiguë de VSPPC a réduit le volume d’AVC et de FÉVG chez les patients atteints d’ICC stable présentant une AOS. Par contre, une thérapie de sept semaines par VSPPC a amélioré la fonction systolique ventriculaire gauche mais n’a pas influé sur la fonction diastolique ou les pressions de remplissage. Les répercussions cliniques potentielles des effets divergents de la thérapie par VSPPC sur la fonction systolique et diastolique ventriculaire gauche chez les patients atteints d’ICC présentant une AOS méritent des études plus approfondies.
Figures

Similar articles
-
Left ventricular systolic and diastolic function in obstructive sleep apnea: impact of continuous positive airway pressure therapy.Circ Heart Fail. 2012 Mar 1;5(2):226-33. doi: 10.1161/CIRCHEARTFAILURE.111.964106. Epub 2012 Mar 13. Circ Heart Fail. 2012. PMID: 22414938
-
Effect of CPAP on diastolic function in coronary artery disease patients with nonsleepy obstructive sleep apnea: A randomized controlled trial.Int J Cardiol. 2017 Aug 15;241:12-18. doi: 10.1016/j.ijcard.2017.03.100. Epub 2017 Mar 25. Int J Cardiol. 2017. PMID: 28408103 Clinical Trial.
-
Tissue Doppler imaging adds incremental value in predicting exercise capacity in patients with congestive heart failure.Heart Vessels. 2007 Jul;22(4):237-44. doi: 10.1007/s00380-006-0961-x. Epub 2007 Jul 20. Heart Vessels. 2007. PMID: 17653517
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
Sleep Apnea as a Risk Factor for Diastolic Dysfunction: A Systematic Review and Meta-Analysis.Respiration. 2022;101(11):1051-1068. doi: 10.1159/000525782. Epub 2022 Aug 30. Respiration. 2022. PMID: 36041415
Cited by
-
Impact of continuous positive airway pressure treatment on left ventricular ejection fraction in patients with obstructive sleep apnea: a meta-analysis of randomized controlled trials.PLoS One. 2013 May 1;8(5):e62298. doi: 10.1371/journal.pone.0062298. Print 2013. PLoS One. 2013. PMID: 23650511 Free PMC article.
-
Obstructive Sleep Apnea in Heart Failure: Review of Prevalence, Treatment with Continuous Positive Airway Pressure, and Prognosis.Tex Heart Inst J. 2018 Jun 1;45(3):151-161. doi: 10.14503/THIJ-15-5678. eCollection 2018 Jun. Tex Heart Inst J. 2018. PMID: 30072851 Free PMC article. Review.
-
Effect of continuous positive pressure ventilation on left ventricular diastolic function E/A ratio in patients with obstructive sleep apnea: a meta-analysis.Sleep Breath. 2023 Dec;27(6):2333-2340. doi: 10.1007/s11325-023-02836-x. Epub 2023 May 10. Sleep Breath. 2023. PMID: 37160854
-
Model-based stability assessment of ventilatory control in overweight adolescents with obstructive sleep apnea during NREM sleep.J Appl Physiol (1985). 2016 Jul 1;121(1):185-97. doi: 10.1152/japplphysiol.01081.2015. Epub 2016 May 12. J Appl Physiol (1985). 2016. PMID: 27174926 Free PMC article.
-
Noninvasive Positive Pressure Ventilation in Chronic Heart Failure.Can Respir J. 2016;2016:3915237. doi: 10.1155/2016/3915237. Epub 2016 Nov 6. Can Respir J. 2016. PMID: 27891061 Free PMC article. Review.
References
-
- Bradley TD, Floras JS. Sleep apnea and heart failure: Part I: Obstructive sleep apnea. Circulation. 2003;107:1671–8. - PubMed
-
- Bradley TD, Floras JS. Sleep apnea and heart failure: Part II: Central sleep apnea. Circulation. 2003;107:1822–6. - PubMed
-
- Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med. 1999;160:1101–6. - PubMed
-
- Javaheri S, Parker TJ, Liming JD, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation. 1998;97:2154–9. - PubMed
-
- Malhotra A, White DP. Obstructive sleep apnoea. Lancet. 2002;360:237–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
