

Ischemic stroke: a cardiovascular risk equivalent? Lessons learned from the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial
- PMID: 18787721
- PMCID: PMC2643176
- DOI: 10.1016/s0828-282x(08)70669-x
Ischemic stroke: a cardiovascular risk equivalent? Lessons learned from the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial
Abstract
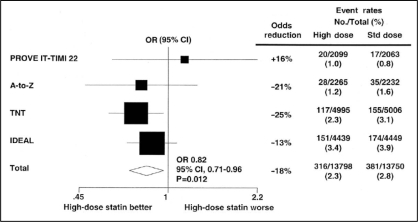
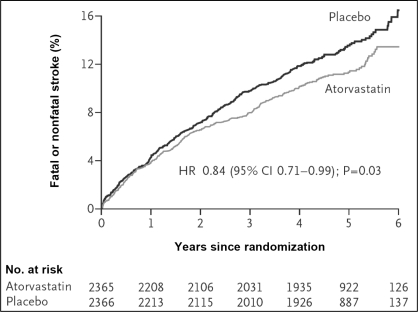
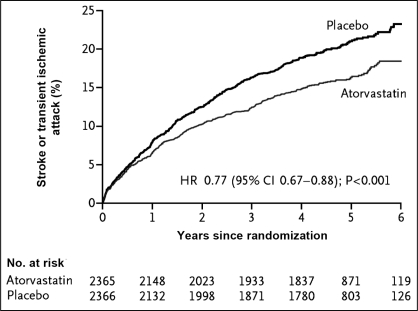
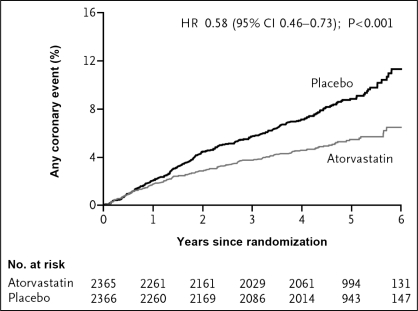
Statin therapy in patients with coronary artery disease or in those at risk for cardiovascular disease is associated with a reduced incidence of ischemic stroke. The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial showed treatment with atorvastatin 80 mg daily in patients with a recent stroke or transient ischemic attack (TIA) reduces the incidence of fatal and nonfatal stroke by 16%. In this population with a recent stroke or TIA, coronary artery disease events and the need for revascularization were a frequent occurrence. Furthermore, the relative reduction of noncerebrovascular events and the need for revascularization was greater with atorvastatin than the reduction of stroke. A patient with a recent ischemic stroke or TIA is at high risk for fatal and nonfatal coronary events (approximately 4% per year), and according to most guidelines for the management of coronary artery disease, such patients should be in the high risk category. Consequently, ischemic stroke should be considered to be a coronary risk equivalent with a prognosis similar to that of a patient with coronary artery disease. Furthermore, both the stroke and coronary artery disease prognoses are improved by treatment with atorvastatin 80 mg daily.
Une thérapie aux statines chez les patients atteints d’une coronaropathie ou vulnérables à une maladie cardiovasculaire s’associe à une diminution de l’incidence d’accidents ischémiques cérébraux. L’essai SPARCL sur la prévention des accidents vasculaires cérébraux (AVC) par réduction énergique des taux de cholestérol a révélé qu’un traitement quotidien de 80 mg d’atorvastatine chez des patients qui avaient récemment subi un AVC ou un accident ischémique transitoire (AIT) réduit de 16 % l’incidence d’AVC fatal ou non fatal. Au sein de cette population ayant récemment subi un AVC ou un AIT, les événements reliés à la coronaropathie et la nécessité de revascularisation étaient courants. De plus, la réduction relative d’événements non vasculaires cérébraux et la nécessité de revascularisation étaient plus élevées avec l’atorvastatine que la réduction des AVC. Un patient ayant récemment subi un AVC ou un AIT court un risque élevé d’événement coronarien fatal ou non fatal (environ 4 % par année), et d’après la plupart des lignes directrices sur la prise en charge des coronaropathies, ces patients devraient faire partie de la catégorie à haut risque. Par conséquent, les accidents ischémiques cérébraux devraient être considérés comme un risque coronarien équivalent, au pronostic similaire à celui du patient atteint d’une coronaropathie. De plus, tant le pronostic d’AVC que celui de coronaropathie s’améliorent grâce à un traitement quotidien de 80 mg d’atorvastatine.
Figures
Similar articles
-
High-dose atorvastatin after stroke or transient ischemic attack: The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators.J Cardiometab Syndr. 2008 Winter;3(1):68-9. doi: 10.1111/j.1559-4572.2008.07967.x. J Cardiometab Syndr. 2008. PMID: 18326981 No abstract available.
-
Atorvastatin reduces the risk of cardiovascular events in patients with carotid atherosclerosis: a secondary analysis of the Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) trial.Stroke. 2008 Dec;39(12):3297-302. doi: 10.1161/STROKEAHA.108.516450. Epub 2008 Oct 9. Stroke. 2008. PMID: 18845807
-
High-dose atorvastatin after stroke or transient ischemic attack.N Engl J Med. 2006 Aug 10;355(6):549-59. doi: 10.1056/NEJMoa061894. N Engl J Med. 2006. PMID: 16899775 Clinical Trial.
-
Atorvastatin: its clinical role in cerebrovascular prevention.Drugs. 2007;67 Suppl 1:55-62. doi: 10.2165/00003495-200767001-00006. Drugs. 2007. PMID: 17910521 Review.
-
Atorvastatin in prevention of stroke and transient ischaemic attack.Expert Opin Pharmacother. 2007 Nov;8(16):2789-97. doi: 10.1517/14656566.8.16.2789. Expert Opin Pharmacother. 2007. PMID: 17956199 Review.
Cited by
-
Atorvastatin in stroke: a review of SPARCL and subgroup analysis.Vasc Health Risk Manag. 2010 Apr 15;6:229-36. doi: 10.2147/vhrm.s6795. Vasc Health Risk Manag. 2010. PMID: 20407630 Free PMC article.
-
Description of the Risk Factors for Ischemic Stroke in the Lebanese Population: Their Association with Age at First Stroke Incidence and the Predictors of Recurrence.J Clin Med. 2025 Mar 17;14(6):2034. doi: 10.3390/jcm14062034. J Clin Med. 2025. PMID: 40142843 Free PMC article.
-
Beyond the Limits: Clinical Utility of Novel Cardiac Biomarkers.Biomed Res Int. 2015;2015:187384. doi: 10.1155/2015/187384. Epub 2015 Oct 4. Biomed Res Int. 2015. PMID: 26504786 Free PMC article. Review.
References
-
- Cholesterol, diastolic blood pressure, and stroke: 13,000 strokes in 450,000 people in 45 prospective cohorts. Prospective studies collaboration. Lancet. 1995;346:1647–53. - PubMed
-
- Iso H, Jacobs DR, Jr, Wentworth D, Neaton JD, Cohen JD. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J Med. 1989;320:904–10. - PubMed
-
- Tirschwell DL, Smith NL, Heckbert SR, Lemaitre RN, Longstreth WT, Jr, Psaty BM. Association of cholesterol with stroke risk varies in stroke subtypes and patient subgroups. Neurology. 2004;63:1868–75. - PubMed
-
- Walldius G, Aastveit AH, Jungner I. Stroke mortality and the apoB/apoA-I ratio: Results of the AMORIS prospective study. J Intern Med. 2006;259:259–66. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
