

Abdominal obesity and the metabolic syndrome: a surgeon's perspective
- PMID: 18787732
- PMCID: PMC2794452
- DOI: 10.1016/s0828-282x(08)71045-6
Abdominal obesity and the metabolic syndrome: a surgeon's perspective
Abstract
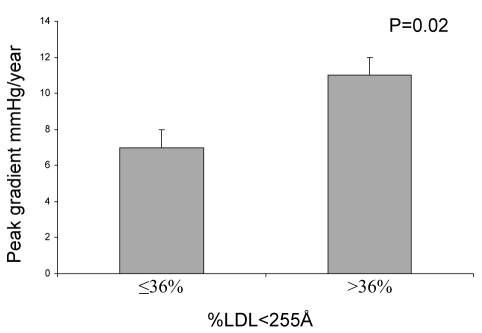
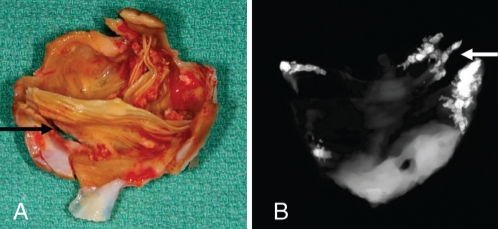
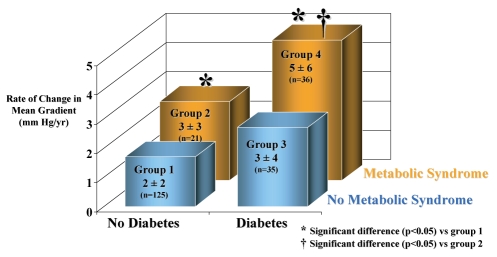
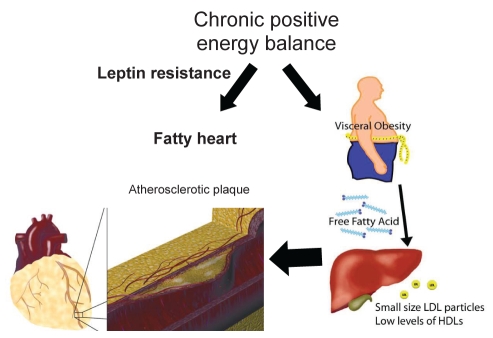
Over the past decade, a major shift in the clinical risk factors in the population undergoing a cardiac surgery has been observed. In the general population, an increasing prevalence of obesity has largely contributed to the development of cardiovascular disorders. Obesity is a heterogeneous condition in which body fat distribution largely determines metabolic perturbations. Consequently, individuals characterized by increased abdominal fat deposition and the so-called metabolic syndrome (MetS) have a higher risk of developing coronary artery disease. Recent studies have also emphasized that visceral obesity is a strong risk factor for the development of heart valve diseases. In fact, individuals characterized by visceral obesity and its metabolic consequences, such as the small dense low-density lipoprotein phenotype, have a faster progression rate of aortic stenosis, which is related to increased valvular inflammation. Furthermore, the degenerative process of implanted bioprostheses is increased in subjects with the MetS and/or diabetes, suggesting that a process akin to atherosclerosis could be involved in the failure of bioprostheses. In addition to being an important risk factor for the development of cardiovascular disorders, the MetS is increasing the operative mortality risk following coronary artery bypass graft surgery. Thus, recent evidence supports visceral obesity as a global risk factor that is affecting the development of many heart disorders, and that is also impacting negatively on the results of patients undergoing surgical treatment for cardiovascular diseases. In the present paper, recent concepts surrounding the MetS and its implications in various cardiovascular disorders are reviewed along with the clinical implications.
Depuis dix ans, on observe un changement majeur des facteurs de risque cliniques de la population qui subit une chirurgie cardiaque. Au sein de la population générale, la prévalence croissante d’obésité a largement contribué à l’apparition de troubles cardiovasculaires. L’obésité est un trouble hétérogène selon lequel la distribution de l’adiposité détermine en grande partie les perturbations métaboliques. Par conséquent, les personnes caractérisées par une augmentation des dépôts de gras abdominal et ce qu’on appelle le syndrome métabolique (SM) courent un plus grand risque de coronaropathie. Des études récentes soulignent également que l’obésité viscérale est un important facteur de risque de maladies valvulaires. En fait, les personnes caractérisées par une obésité viscérale et ses conséquences métaboliques, telles que le phénotype à lipoprotéine de basse densité à la fois petit et dense, présentent un taux d’évolution plus rapide de sténose aortique, relié à un accroissement de l’inflammation valvulaire. En outre, le processus dégénératif des bioprothèses implantées augmente chez les sujets atteints du SM ou du diabète, ce qui laisse supposer qu’un processus semblable à l’athérosclérose pourrait contribuer à l’échec des bioprothèses. En plus d’être un facteur de risque important d’apparition des troubles cardiovasculaires, le SM accroît le risque de mortalité opératoire après un pontage aortocoronarien. Ainsi, les données probantes récentes étayent que l’obésité viscérale est un facteur de risque global qui influe sur l’apparition de nombreux troubles cardiaques, ce qui nuit aux résultats des patients qui subissent un traitement chirurgical en raison d’une maladie cardiovasculaire. Dans le présent article, l’auteur analyse les concepts récents entourant le SM et ses conséquences pour divers troubles cardiovasculaires ainsi que les répercussions cliniques de ces concepts.
Figures
References
-
- Zimmet P. Diabesity – the biggest epidemic in human history. MedGenMed. 2007;9:39.
-
- Brochu M, Starling RD, Tchernof A, Matthews DE, Garcia-Rubi E, Poehlman ET. Visceral adipose tissue is an independent correlate of glucose disposal in older obese postmenopausal women. J Clin Endocrinol Metab. 2000;85:2378–84. - PubMed
-
- Després JP, Lemieux I. Abdominal obesity and metabolic syndrome. Nature. 2006;444:881–7. - PubMed
-
- Zimmet P, Magliano D, Matsuzawa Y, Alberti G, Shaw J. The metabolic syndrome: A global public health problem and a new definition. J Atheroscler Thromb. 2005;12:295–300. - PubMed
-
- Unger RH. Longevity, lipotoxicity and leptin: The adipocyte defense against feasting and famine. Biochimie. 2005;87:57–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
