

Imaging amyloid deposition in Lewy body diseases
- PMID: 18794492
- PMCID: PMC2637553
- DOI: 10.1212/01.wnl.0000326146.60732.d6
Imaging amyloid deposition in Lewy body diseases
Abstract
Background: Extrapyramidal motor symptoms precede dementia in Parkinson disease (PDD) by many years, whereas dementia occurs early in dementia with Lewy bodies (DLB). Despite this clinical distinction, the neuropsychological and neuropathologic features of these conditions overlap. In addition to widespread distribution of Lewy bodies, both diseases have variable burdens of neuritic plaques and neurofibrillary tangles characteristic of Alzheimer disease (AD).
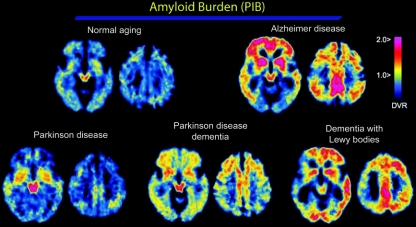
Objectives: To determine whether amyloid deposition, as assessed by PET imaging with the beta-amyloid-binding compound Pittsburgh Compound B (PiB), can distinguish DLB from PDD, and to assess whether regional patterns of amyloid deposition correlate with specific motor or cognitive features.
Methods: Eight DLB, 7 PDD, 11 Parkinson disease (PD), 15 AD, and 37 normal control (NC) subjects underwent PiB-PET imaging and neuropsychological assessment. Amyloid burden was quantified using the PiB distribution volume ratio.
Results: Cortical amyloid burden was higher in the DLB group than in the PDD group, comparable to the AD group. Amyloid deposition in the PDD group was low, comparable to the PD and NC groups. Relative to global cortical retention, occipital PiB retention was lower in the AD group than in the other groups. For the DLB, PDD, and PD groups, amyloid deposition in the parietal (lateral and precuneus)/posterior cingulate region was related to visuospatial impairment. Striatal PiB retention in the DLB and PDD groups was associated with less impaired motor function.
Conclusions: Global cortical amyloid burden is high in dementia with Lewy bodies (DLB) but low in Parkinson disease dementia. These data suggest that beta-amyloid may contribute selectively to the cognitive impairment of DLB and may contribute to the timing of dementia relative to the motor signs of parkinsonism.
Figures

References
-
- Emre M, Aarsland D, Brown R, et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov Disord 2007;22:1689–1707. - PubMed
-
- McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 2005;65:1863–1872. - PubMed
-
- Lippa CF, Duda JE, Grossman M, et al. DLB/PDD Working Group. DLB and PDD boundary issues: diagnosis, treatment, molecular pathology, and biomarkers. Neurology 2007;68:812–819. - PubMed
-
- Harding AJ, Halliday GM. Cortical Lewy body pathology in the diagnosis of dementia. Acta Neuropathol 2001;102:355–363. - PubMed
-
- Tiraboschi P, Hansen LA, Alford M, et al. Cholinergic dysfunction in diseases with Lewy bodies. Neurology 2000;54:407–411. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical