

Treatment and survival differences in older Medicare patients with lung cancer as compared with those who are dually eligible for Medicare and Medicaid
- PMID: 18794546
- PMCID: PMC2652096
- DOI: 10.1200/JCO.2008.16.3071
Treatment and survival differences in older Medicare patients with lung cancer as compared with those who are dually eligible for Medicare and Medicaid
Abstract
Purpose: This study compares non-small-cell lung cancer (NSCLC) treatments provided to older patients (age > or = 66 years) who are dually eligible for Medicare and Medicaid with treatments provided to similar patients who are insured by Medicare. We extend the analysis to include a comparison of survival rates between Medicare and dually eligible patients. Dual eligibility is associated with low socioeconomic status. However, Medicaid coverage in addition to Medicare removes many financial barriers to care.
Patients and methods: The sample included 2,626 older patients with local and regional stage NSCLC diagnosed between 1997 and 2000. Four outcomes were studied: the likelihood of receiving resection, chemotherapy, radiation therapy, and survival (perioperative and longer-term). Logistic regression was used to predict the likelihood of treatment, and stratified and multivariate analyses were used to evaluate differences in survival.
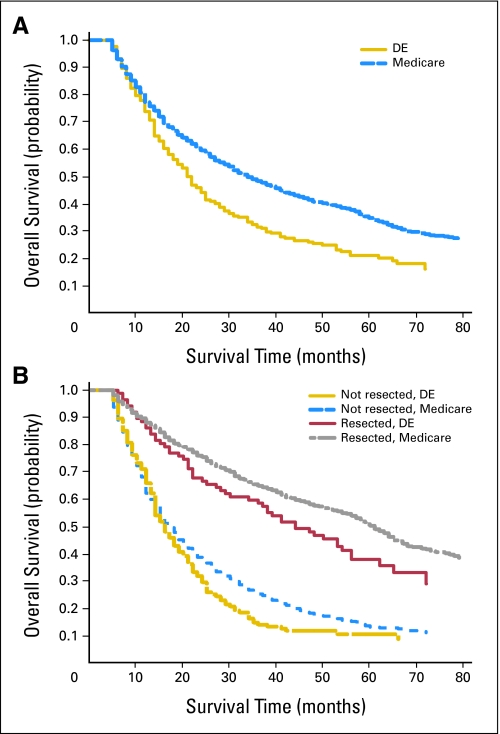
Results: Dually eligible patients were half as likely to undergo resection as Medicare patients (P < .001) and were more likely to receive radiation than Medicare patients. Stratified and multivariate analyses showed that surgically treated dually eligible patients had slightly inferior survival as compared with that of Medicare patients. Survival was equivalent among patients who did not undergo resection, regardless of insurance coverage.
Conclusion: Older dually eligible patients with NSCLC had a lower likelihood of undergoing resection despite controls for socioeconomic factors and comorbidities. However, if such patients were surgically treated, survival improved substantially, but it remained inferior to the survival of Medicare patients. Additional research is needed to understand why resection rates were substantially lower among dually eligible patients.
Figures
References
-
- Edwards B, Brown M, Wingo P, et al: Annual report to the nation on the status of cancer, 1975-2002, featuring population-based trends in cancer treatment. J Natl Cancer Inst 97:1407-1427, 2005 - PubMed
-
- Sullivan V, Tran T, Holmstrom A, et al: Advanced age does not exclude lobectomy for non-small cell lung carcinoma. Chest 128:2671-2676, 2005 - PubMed
-
- Winton T, Livingston R, Johnson D, et al: Vinorelbine plus cisplatin vs. observation in resected non-small cell lung cancer. N Engl J Med 352:2589-2597, 2005 - PubMed
-
- Arriagada R, Bergman B, Dunant A, et al: Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small cell lung cancer. N Engl J Med 350:351-360, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
