

Five-year follow-up of patients with advanced chronic lymphocytic leukemia treated with allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning
- PMID: 18794548
- PMCID: PMC2652085
- DOI: 10.1200/JCO.2007.15.4757
Five-year follow-up of patients with advanced chronic lymphocytic leukemia treated with allogeneic hematopoietic cell transplantation after nonmyeloablative conditioning
Abstract
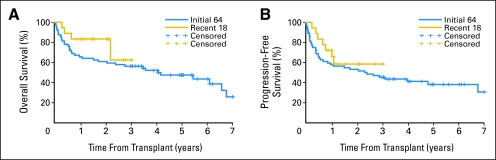
Purpose: We reported encouraging early results of allogeneic hematopoietic cell transplantation (HCT) after nonmyeloablative conditioning in 64 patients who had advanced chronic lymphocytic leukemia (CLL). Here, we have extended the follow-up to a median of 5 years and have included data on an additional 18 patients.
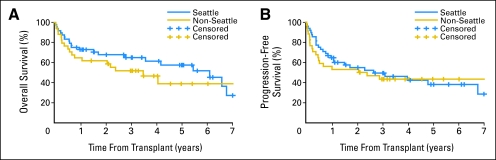
Patients and methods: Eighty-two patients, age 42 to 72 years, who had fludarabine-refractory CLL were conditioned with 2 Gy total-body irradiation alone or combined with fludarabine followed by HCT from related (n = 52) or unrelated (n = 30) donors.
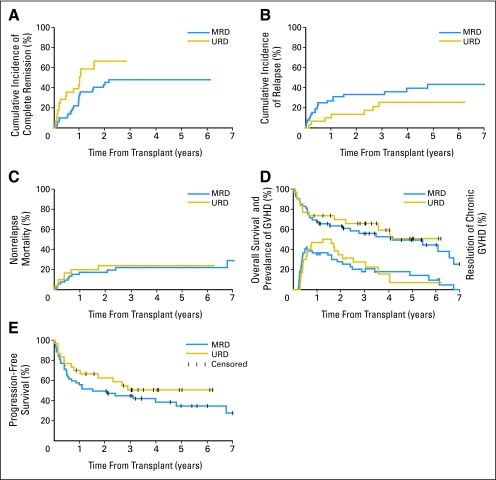
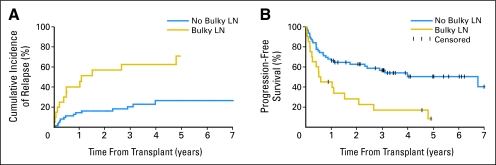
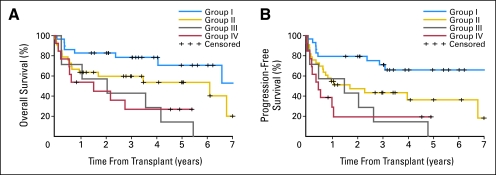
Results: Complete remission (CR) and partial remission were achieved in 55% and 15% of patients, respectively. Higher CR rates were noted after unrelated HCT (67% v 48%). The 5-year incidences of nonrelapse mortality (NRM), progression/relapse, overall survival, and progression-free survival were 23%, 38%, 50%, and 39%, respectively. Among 25 patients initially reported in CR, 8% relapsed and 8% died as a result of NRM, whereas 84% have remained alive and in CR. Among 14 responding patients who were tested and who had molecular eradication of their disease, two died as a result of NRM, two relapsed, and 10 have remained negative. At 5 years, 76% of living patients were entirely well, whereas 24% continued to receive immunosuppression for chronic graft-versus-host disease; the median performance status in each group was 100% and 90%, respectively. Lymphadenopathy > or = 5 cm, but not cytogenetic abnormalities at HCT, predicted relapse. In a risk-stratification model, patients who had lymphadenopathy less than 5 cm and no comorbidities had a 5-year OS of 71%.
Conclusion: Nonmyeloablative HCT resulted in a median survival of 5 years for patients who had fludarabine-refractory CLL with sustained remissions and in the continued resolution of chronic graft-versus-host disease in surviving patients.
Figures
Comment in
-
Role of allogeneic hematopoietic stem-cell transplantation in chronic lymphocytic leukemia.J Clin Oncol. 2008 Oct 20;26(30):4864-5. doi: 10.1200/JCO.2008.17.7733. Epub 2008 Sep 15. J Clin Oncol. 2008. PMID: 18794537 No abstract available.
References
-
- Esteve J, Montserrat E, Dreger P, et al: Stem cell transplantation (SCT) for chronic lymphocytic leukemia (CLL): Outcome and prognostic factors after autologous and allogeneic transplants. Blood 98:482a, 2001. (abstr 2013)
-
- Bottcher S, Ritgen M, Pott C, et al: Comparative analysis of minimal residual disease detection using four-color flow cytometry, consensus IgH-PCR, and quantitative IgH PCR in CLL after allogeneic and autologous stem cell transplantation. Leukemia 18:1637-1645, 2004 - PubMed
-
- Ritgen M, Stilgenbauer S, von Neuhoff N, et al: Graft-versus-leukemia activity may overcome therapeutic resistance of chronic lymphocytic leukemia with unmutated immunoglobulin variable heavy-chain gene status: Implications of minimal residual disease measurement with quantitative PCR. Blood 104:2600-2602, 2004 - PubMed
-
- Moreno C, Villamor N, Colomer D, et al: Clinical significance of minimal residual disease, as assessed by different techniques, after stem cell transplantation for chronic lymphocytic leukemia. Blood 107:4563-4569, 2006 - PubMed
-
- Michallet M, Archimbaud E, Bandini G, et al: HLA-identical sibling bone marrow transplantation in younger patients with chronic lymphocytic leukemia: European Group for Blood and Marrow Transplantation and the International Bone Marrow Transplant Registry. Ann Intern Med 124:311-315, 1996 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
