

Systematic review: comparative effectiveness and safety of premixed insulin analogues in type 2 diabetes
- PMID: 18794553
- PMCID: PMC4762020
- DOI: 10.7326/0003-4819-149-8-200810210-00242
Systematic review: comparative effectiveness and safety of premixed insulin analogues in type 2 diabetes
Abstract
Background: Evidence comparing premixed insulin analogues (a mixture of rapid-acting and intermediate-acting insulin analogues) with other antidiabetic agents is urgently required to guide appropriate therapy.
Purpose: To summarize the English-language literature on the effectiveness and safety of premixed insulin analogues compared with other antidiabetic agents in adults with type 2 diabetes.
Data sources: The authors searched MEDLINE, EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials from inception to February 2008 and sought unpublished data from the U.S. Food and Drug Administration, European Medicines Agency, and industry.
Study selection: Studies with control groups that compared premixed insulin analogues with another antidiabetic medication in adults with type 2 diabetes.
Data extraction: 2 reviewers using standardized protocols performed serial abstraction.
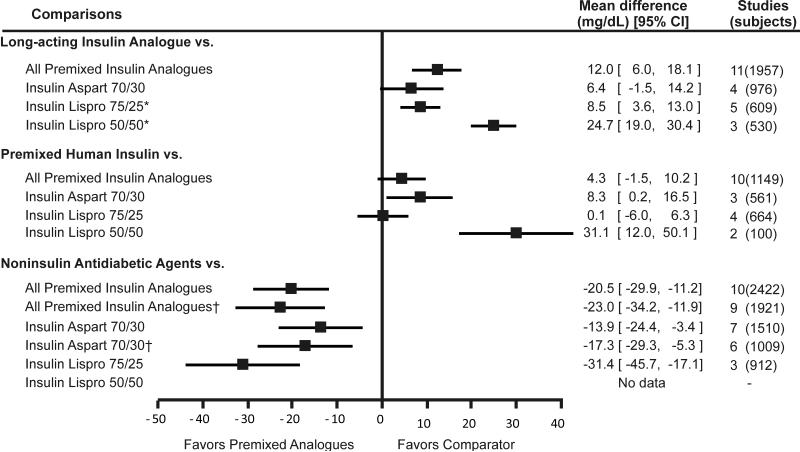
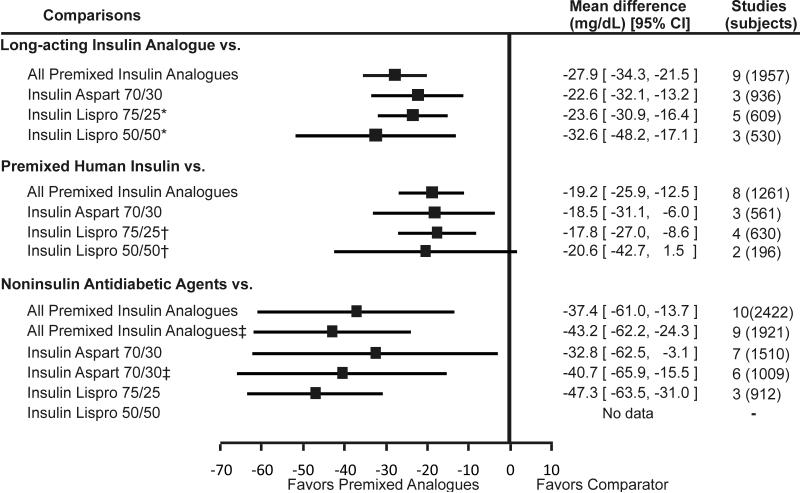
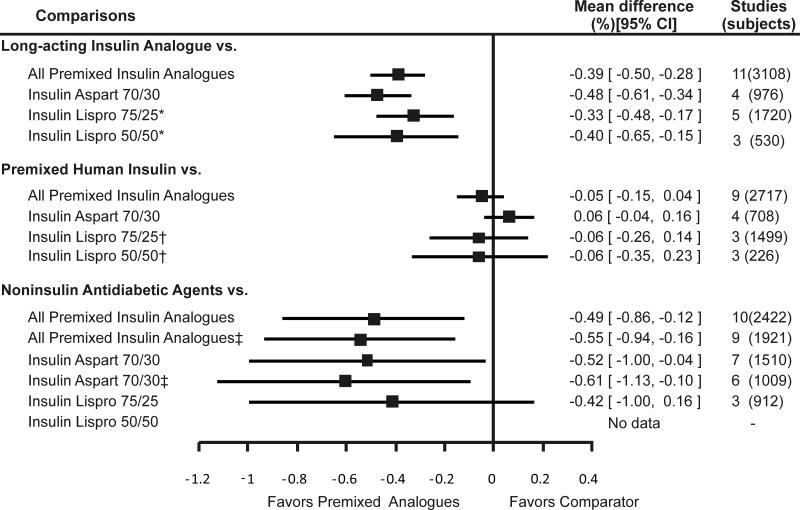
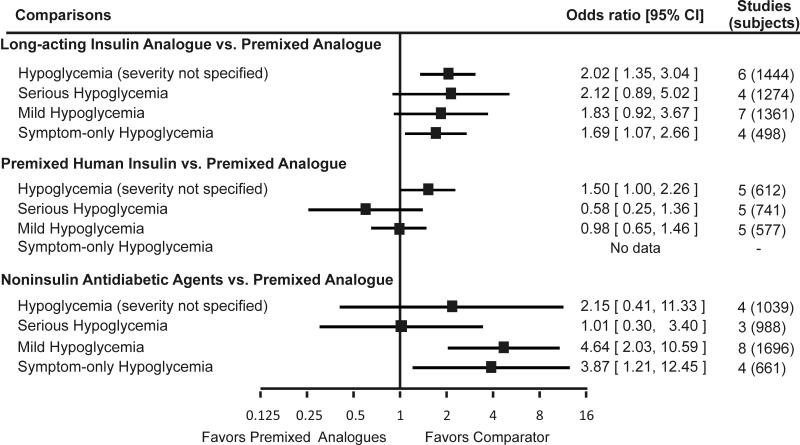
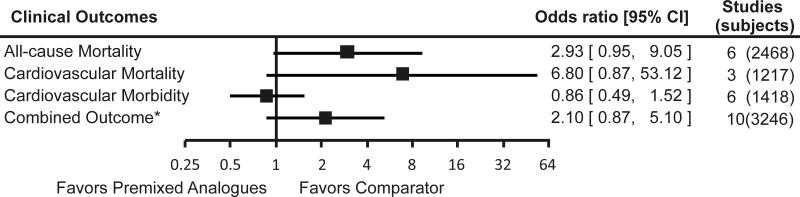
Data synthesis: Evidence from clinical trials was inconclusive for clinical outcomes, such as mortality. Therefore, the review focused on intermediate outcomes. Premixed insulin analogues were similar to premixed human insulin in decreasing fasting glucose levels, hemoglobin A(1c) levels, and the incidence of hypoglycemia but were more effective in decreasing postprandial glucose levels (mean difference, -1.1 mmol/L; 95% CI, -1.4 to -0.7 mmol/L [-19.2 mg/dL; 95% CI, -25.9 to -12.5 mg/dL]). Compared with long-acting insulin analogues, premixed insulin analogues were superior in decreasing postprandial glucose levels (mean difference, -1.5 mmol/L; CI, -1.9 to -1.2 mmol/L [-27.9 mg/dL; CI, -34.3 to -21.5 mg/dL]) and hemoglobin A(1c) levels (mean difference, -0.39% [CI, -0.50% to -0.28%]) but were inferior in decreasing fasting glucose levels (mean difference, 0.7 mmol/L; CI, 0.3 to 1.0 mmol/L [12.0 mg/dL; CI, 6.0 to 18.1 mg/dL]) and were associated with a higher incidence of hypoglycemia. Compared with noninsulin antidiabetic agents, premixed insulin analogues were more effective in decreasing fasting glucose levels (mean difference, -1.1 mmol/L; CI, -1.7 to -0.6 mmol/L [-20.5 mg/dL; CI, -29.9 to -11.2 mg/dL]), postprandial glucose levels (mean difference, -2.1 mmol/L; CI, -3.4 to -0.8 mmol/L [-37.4 mg/dL; CI, -61.0 to -13.7 mg/dL]), and hemoglobin A(1c) levels (mean difference, -0.49% [CI, -0.86% to -0.12%]) but were associated with a higher incidence of hypoglycemia.
Limitations: The literature search was restricted to studies published in English. Data on clinical outcomes were limited. The small number of studies for each comparison limited assessment of between-study heterogeneity.
Conclusion: Premixed insulin analogues provide glycemic control similar to that of premixed human insulin and may provide tighter glycemic control than long-acting insulin analogues and noninsulin antidiabetic agents.
Figures
Comment in
-
Newer insulins in search of a niche.Ann Intern Med. 2008 Oct 21;149(8):586-8. doi: 10.7326/0003-4819-149-8-200810210-00011. Ann Intern Med. 2008. PMID: 18936506 No abstract available.
References
-
- Centers for Disease Control and Prevention . National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Department of Health and Human Services, Centers for Disease Control and Prevention; Atlanta, GA: U.S.: 2005.
-
- Gregg EW, Cadwell BL, Cheng YJ, Cowie CC, Williams DE, Geiss L, et al. Trends in the prevalence and ratio of diagnosed to undiagnosed diabetes according to obesity levels in the U.S. Diabetes Care. 2004;27:2806–12. - PubMed
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837–53. - PubMed
-
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12. - PubMed
-
- Wells GA, Shea B, O’Connel D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2007. [accessed on August 4, 2008]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm Available online at.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical