

Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors
- PMID: 18795210
- PMCID: PMC2556445
- DOI: 10.1900/RDS.2008.5.73
Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors
Abstract
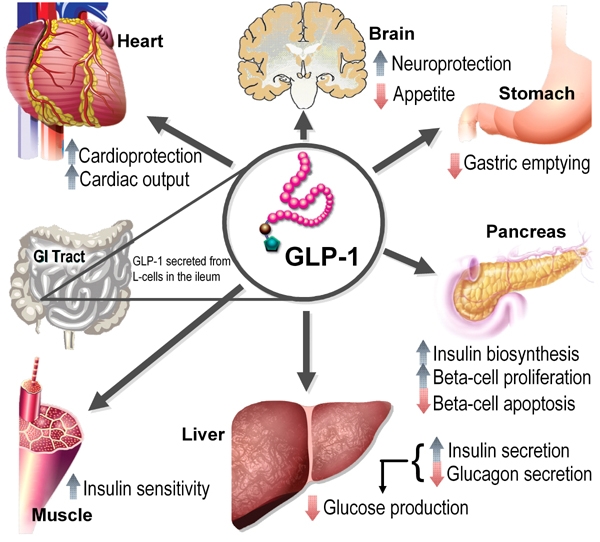
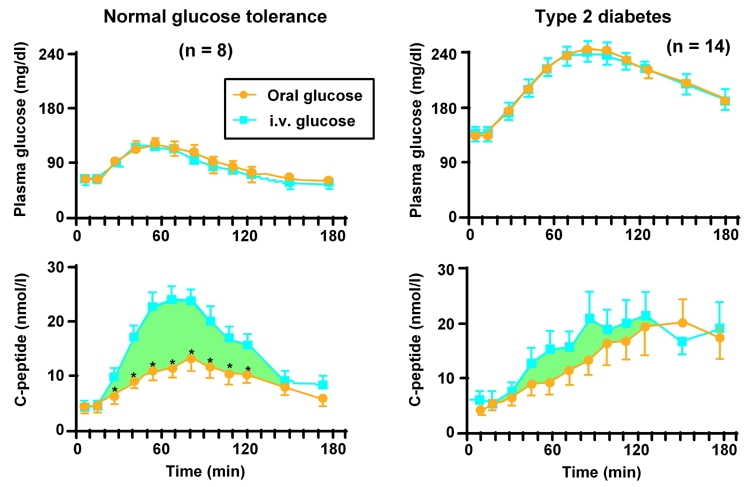
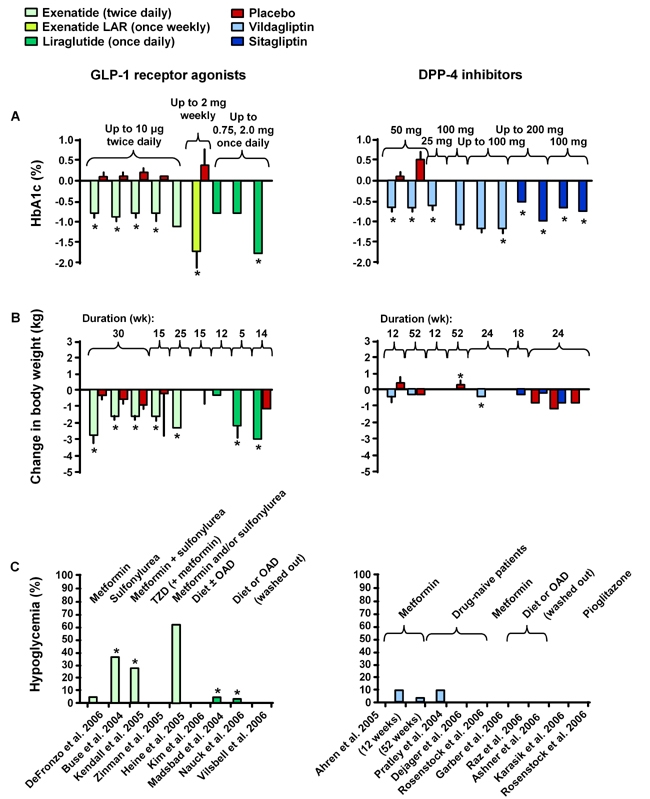
Until recently, the pathogenesis of type 2 diabetes mellitus (T2DM) has been conceptualized in terms of the predominant defects in insulin secretion and insulin action. It is now recognized that abnormalities in other hormones also contribute to the development of hyperglycemia. For example, the incretin effect, mediated by glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP), is attenuated in T2DM. Intravenous administration of GLP-1 ameliorates hyperglycemia in patients with T2DM, but an extremely short half-life limits its utility as a therapeutic agent. Strategies to leverage the beneficial effects of GLP-1 include GLP-1 receptor agonists or analogs or dipeptidyl peptidase-4 (DPP-4) inhibitors-agents that act by slowing the inactivation of endogenous GLP-1 and GIP. The GLP-1 agonist exenatide has been shown to improve HbA1c and decrease body weight. However, exenatide is limited by its relatively short pharmacologic half-life, various gastrointestinal (GI) side effects, and the development of antibodies. Studies of a long-acting exenatide formulation suggest that it has improved efficacy and also promotes weight loss. Another prospect is liraglutide, a once-daily human GLP-1 analog. In phase 2 studies, liraglutide lowered HbA1c by up to 1.7% and weight by approximately 3 kg, with apparently fewer GI side effects than exenatide. DPP-4 inhibitors such as sitagliptin and vildagliptin result in clinically significant reductions in HbA1c, and are weight neutral with few GI side effects. This review will provide an overview of current and emerging agents that augment the incretin system with a focus on the role of GLP-1 receptor agonists and DPP-4 inhibitors.
Figures
References
-
- Aronoff SL, Berkowitz K, Shreiner B, Want L. Glucose metabolism and regulation: beyond insulin and glucagon. Diabetes Spectrum. 2004;17:183–190.
-
- Drucker DJ. The biology of incretin hormones. Cell Metab. 2006;3(3):153–165. - PubMed
-
- Pratley RE, Weyer C. The role of impaired early insulin secretion in the pathogenisis of type II diabetes mellitus. Diabetologia. 2001;44:929–945. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous