

Changes in muscle mass, muscle strength, and power but not physical function are related to testosterone dose in healthy older men
- PMID: 18795988
- PMCID: PMC2585153
- DOI: 10.1111/j.1532-5415.2008.01927.x
Changes in muscle mass, muscle strength, and power but not physical function are related to testosterone dose in healthy older men
Abstract
Objectives: To examine the effect of graded doses of testosterone on physical function and muscle performance in healthy, older men.
Design: Randomized, double-blind, placebo-controlled clinical trial.
Setting: General clinical research center.
Participants: Community-dwelling healthy men aged 60 to 75 (N=44).
Intervention: Monthly treatment with a gonadotropin-releasing hormone agonist plus 25, 50, 125, or 300 mg/wk of intramuscular injections of testosterone enanthate for 20 weeks.
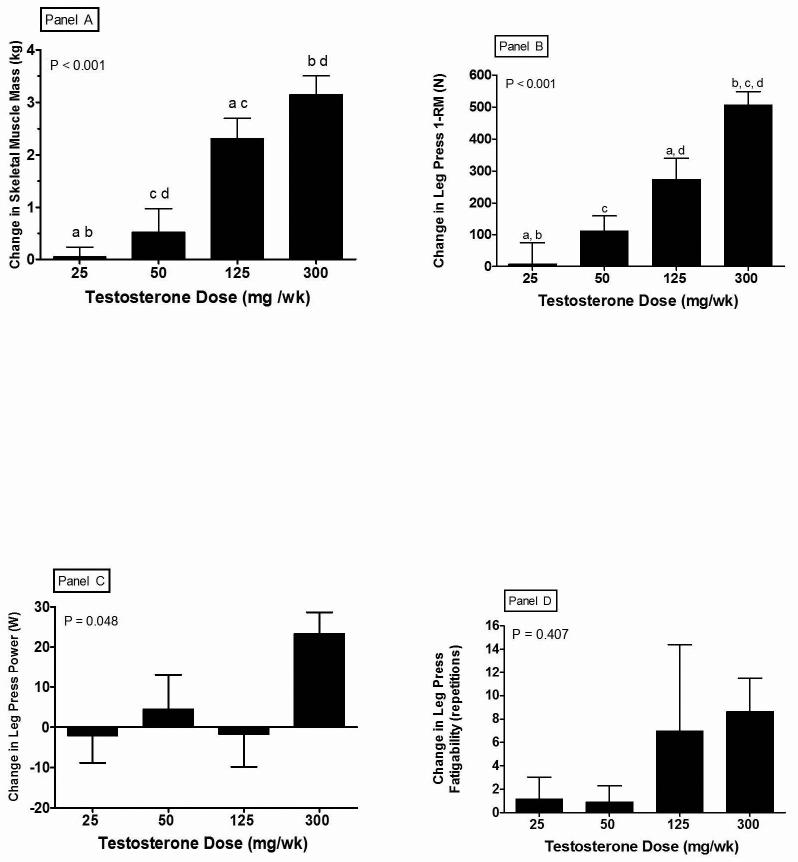
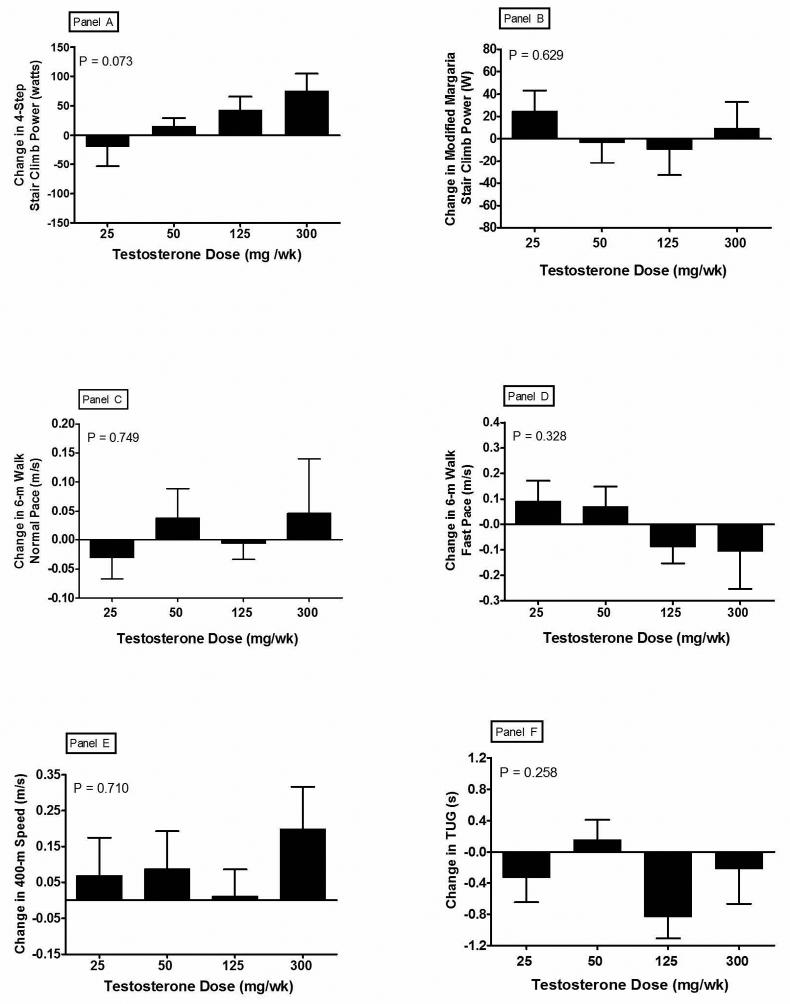
Measurements: Skeletal muscle mass (SMM) was estimated using dual-energy X-ray absorptiometry. Leg press strength was measured by one repetition maximum, leg power by Nottingham Leg Rig, and muscle fatigability by repetitions to failure in the leg press exercise. Stair climbing, 6-meter and 400-meter walking speed, and a timed-up-and-go (TUG) test were used to assess physical function.
Results: Significant testosterone dose- and concentration-dependent increases were observed in SMM (P<.001) and maximal strength (P=.001) but not muscle fatigability. Leg power also increased dose-dependently (P=.048). In contrast, changes in self-selected normal and fast walking speed over 6 or 400 meters, stair climbing power, and time for the TUG were not significantly related to testosterone dose, testosterone concentrations, or changes in muscle strength or power, or SMM.
Conclusion: Testosterone administration was associated with dose-dependent increases in SMM, leg strength, and power but did not improve muscle fatigability or physical function. The observation that physical function scores did not improve linearly with strength suggests that these high-functioning older men were already in the asymptotic region of the curve describing the relationship between physical function and strength.
Figures
References
-
- Baumgartner RN, Waters DL, Gallagher D, et al. Predictors of skeletal muscle mass in elderly men and women. Mech Ageing Dev. 1999;107:123–136. - PubMed
-
- Melton LJ, 3rd, Khosla S, Crowson CS, et al. Epidemiology of sarcopenia. J Am Geriatr Soc. 2000;48:625–630. - PubMed
-
- Roy TA, Blackman MR, Harman SM, et al. Interrelationships of serum testosterone and free testosterone index with FFM and strength in aging men. Am J Physiol Endocrinol Metab. 2002;283:E284–294. - PubMed
-
- Knutzen KM, Brilla L, Caine D, et al. Absolute vs. relative machine strength as predictors of function in older adults. J Strength Cond Res. 2002;16:628–640. - PubMed
-
- Ferrucci L, Guralnik JM, Buchner D, et al. Departures from linearity in the relationship between measures of muscular strength and physical performance of the lower extremities: the Women's Health and Aging Study. J Gerontol A Biol Sci Med Sci. 1997;52:M275–285. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 1R01DK59627-01/DK/NIDDK NIH HHS/United States
- 2R01DK49296-02A/DK/NIDDK NIH HHS/United States
- R01 AG014369/AG/NIA NIH HHS/United States
- R01 DK070534/DK/NIDDK NIH HHS/United States
- P20 RR011145/RR/NCRR NIH HHS/United States
- G12RR03026/RR/NCRR NIH HHS/United States
- R01 DK059627/DK/NIDDK NIH HHS/United States
- R01 DK049296/DK/NIDDK NIH HHS/United States
- U54 HD041748/HD/NICHD NIH HHS/United States
- T32 DK007201/DK/NIDDK NIH HHS/United States
- R01 HD043348/HD/NICHD NIH HHS/United States
- 1R01HD043348-01/HD/NICHD NIH HHS/United States
- U01 AG014369/AG/NIA NIH HHS/United States
- U54HD041748-01/HD/NICHD NIH HHS/United States
- 1R01AG14369-01/AG/NIA NIH HHS/United States
- G12 RR003026/RR/NCRR NIH HHS/United States
- P20RR11145/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
