

ECDI-fixed allogeneic splenocytes induce donor-specific tolerance for long-term survival of islet transplants via two distinct mechanisms
- PMID: 18796615
- PMCID: PMC2567158
- DOI: 10.1073/pnas.0805204105
ECDI-fixed allogeneic splenocytes induce donor-specific tolerance for long-term survival of islet transplants via two distinct mechanisms
Abstract
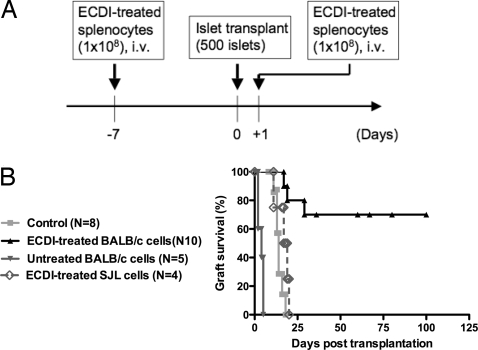
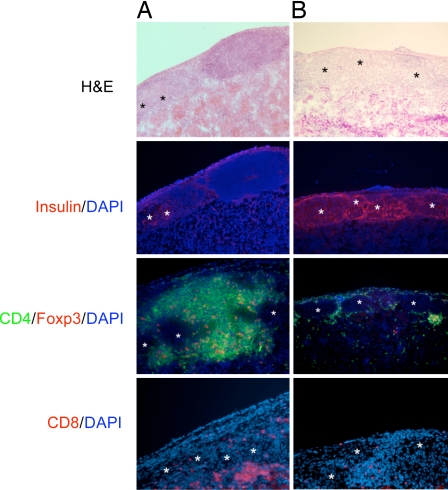
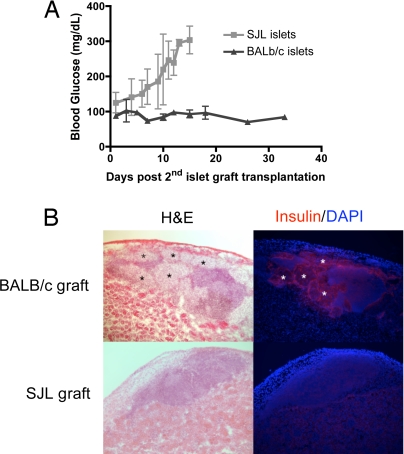
A major challenge for human allogeneic islet transplantation is the development of effective methods to induce donor-specific tolerance to obviate the need for life-long immunosuppression that is toxic to the insulin-producing beta cells and detrimental to the host. We developed an efficient donor-specific tolerance therapy that utilizes infusions of ethylene carbodiimide (ECDI)-treated donor splenic antigen-presenting cells that results in indefinite survival of allogeneic islet grafts in the absence of immunosuppression. Furthermore, we show that induction of tolerance is critically dependent on synergistic effects between an intact programmed death 1 receptor-programmed death ligand 1 signaling pathway and CD4(+)CD25(+)Foxp3(+) regulatory T cells. This highly efficient antigen-specific therapy with a complete avoidance of immunosuppression has significant therapeutic potential in human islet cell transplantation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Shapiro AM, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med. 2006;355:1318–1330. - PubMed
-
- Ryan EA, et al. Five-year follow-up after clinical islet transplantation. Diabetes. 2005;54:2060–2069. - PubMed
-
- Mohanakumar T, et al. A significant role for histocompatibility in human islet transplantation. Transplantation. 2006;82:180–187. - PubMed
-
- Campbell PM, et al. High risk of sensitization after failed islet transplantation. Am J Transplant. 2007;7:2311–2317. - PubMed
-
- Lobo PI, et al. Development of anti-human leukocyte antigen class 1 antibodies following allogeneic islet cell transplantation. Transplant Proc. 2005;37:3438–3440. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
