

Popcorn calcification in osteogenesis imperfecta: incidence, progression, and molecular correlation
- PMID: 18798308
- PMCID: PMC6320686
- DOI: 10.1002/ajmg.a.32508
Popcorn calcification in osteogenesis imperfecta: incidence, progression, and molecular correlation
Abstract
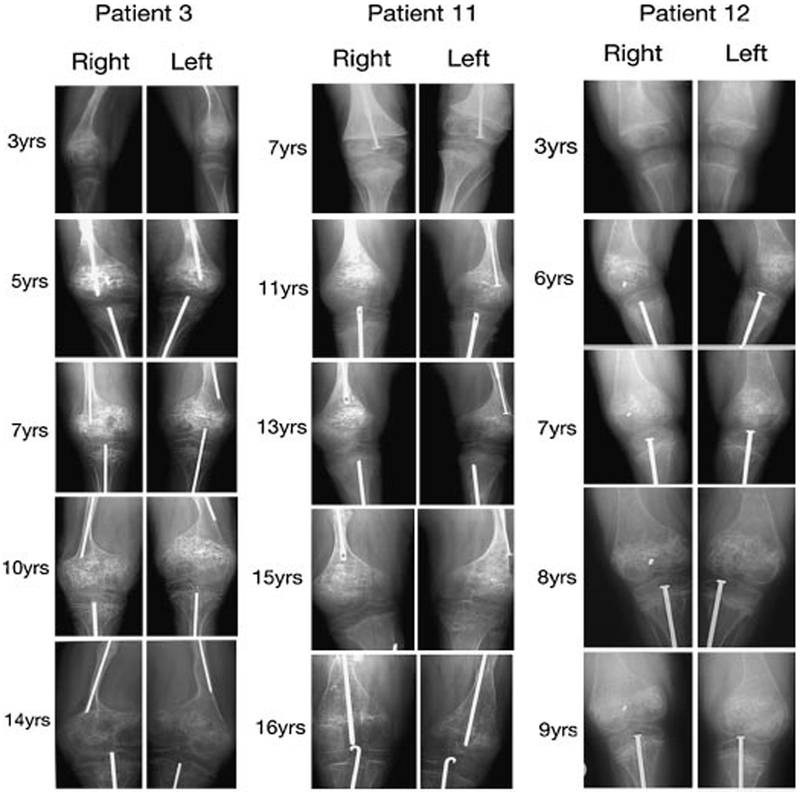
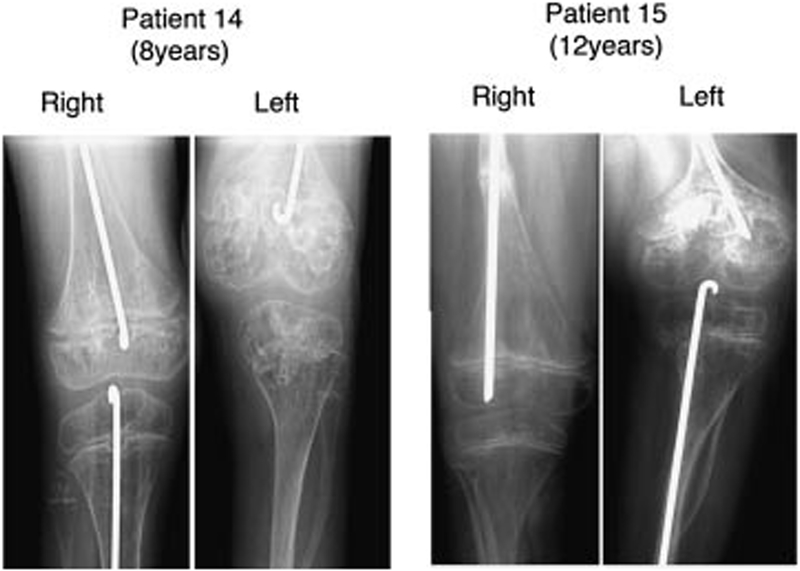
Osteogenesis imperfecta (OI) is a heritable disorder characterized by osteoporosis and increased susceptibility to fracture. All children with severe OI have extreme short stature and some have "popcorn" calcifications, areas of disorganized hyperdense lines in the metaphysis and epiphysis around the growth plate on lower limb radiographs. Popcorn calcifications were noted on radiographs of two children with non-lethal type VIII OI, a recessive form caused by P3H1 deficiency. To determine the incidence, progression, and molecular correlations of popcorn calcifications, we retrospectively examined serial lower limb radiographs of 45 children with type III or IV OI and known dominant mutations in type I collagen. Popcorn calcifications were present in 13 of 25 type III (52%), but only 2 of 20 type IV (10%), OI children. The mean age of onset was 7.0 years, with a range of 4-14 years. All children with popcorn calcifications had this finding in their distal femora, and most also had calcifications in proximal tibiae. While unilateral popcorn calcification contributes to femoral growth deficiency and leg length discrepancy, severe linear growth deficiency, and metaphyseal flare do not differ significantly between type III OI patients with and without popcorn calcifications. The type I collagen mutations associated with popcorn calcifications occur equally in both COL1A1 and COL1A2, and have no preferential location along the chains. These data demonstrate that popcorn calcifications are a frequent feature of severe OI, but do not distinguish cases with defects in collagen structure (primarily dominant type III OI) or modification (recessive type VIII OI).
Copyright 2008 Wiley-Liss, Inc.
Figures
References
-
- Baldridge D, Schwarze U, Morello R, Lennington J, Bertin TK, Pace JM, Pepin MG, Weis M, Eyre DR, Walsh J, Lambert D, Green A, Robinson H, Michelson M, Houge G, Lindman C, Martin J, Ward J, Lemyre E, Mitchell JJ, Krakow D, Rimoin DL, Cohn DH, Byers PH, Cole WG, Lee B. 2008. CRTAP and LEPRE1 mutations in recessive osteogenesis imperfecta Hum Mutat (in press). - PMC - PubMed
-
- Barnes AM, Chang W, Morello R, Cabral WA, Weis M, Eyre DR, Leikin S, Makareeva E, Kuznetsova N, Uveges TE, Ashok A, Flor AW, Mulvihill JJ, Wilson PL, Sundaram UT, Lee B, Marini JC. 2006. Deficiency of cartilage-associated protein in recessive lethal osteogenesis imperfecta. N Engl J Med 355: 2757–2764. - PMC - PubMed
-
- Brenner RE, Schiller B, Pontz BF, Lehmann H, Teller WM, Spranger J, Vetter U. 1993. Osteogenesis imperfecta in childhood and adolescence. Monatsschr Kinderheilkd 141: 940–945. - PubMed
-
- Bullough PG, Davidson DD, Lorenzo JC. 1981. The morbid anatomy of the skeleton in osteogenesis imperfecta. Clin Orthop Relat Res 159:42–57. - PubMed
-
- Byers PH, Cole WG. 2002. Osteogenesis imperfecta In: Royce PM, Steinman B, editors. Connective tissue and its heritable disorders. 2nd edition New York: Wiley-Liss, Inc. p 385–430.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
