

Therapeutic advances in leukemia and myelodysplastic syndrome over the past 40 years
- PMID: 18798533
- PMCID: PMC4392892
- DOI: 10.1002/cncr.23655
Therapeutic advances in leukemia and myelodysplastic syndrome over the past 40 years
Abstract
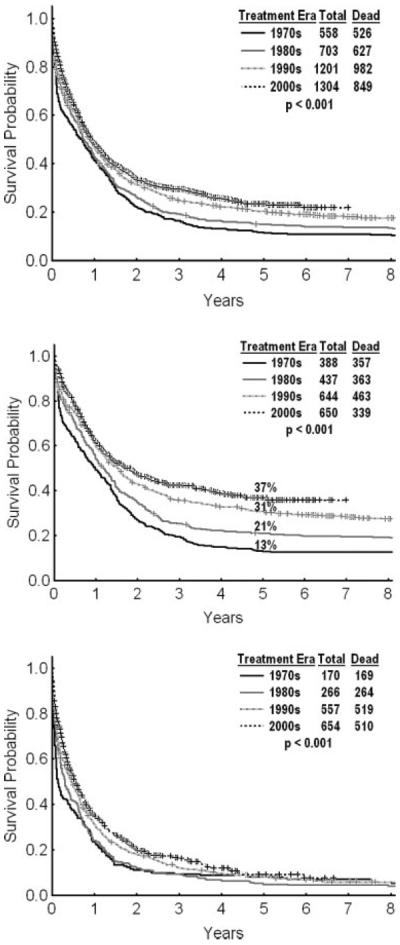
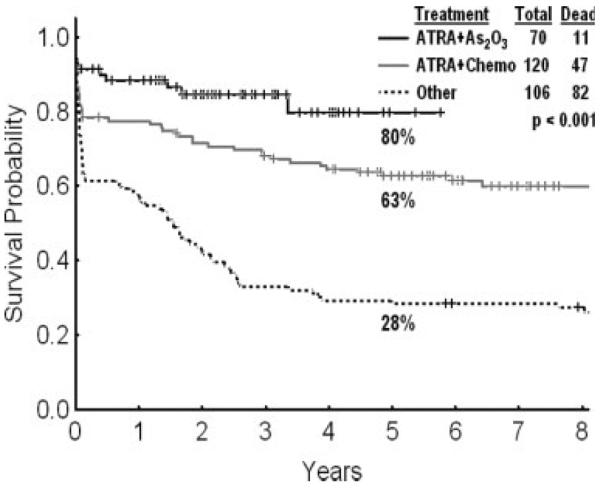
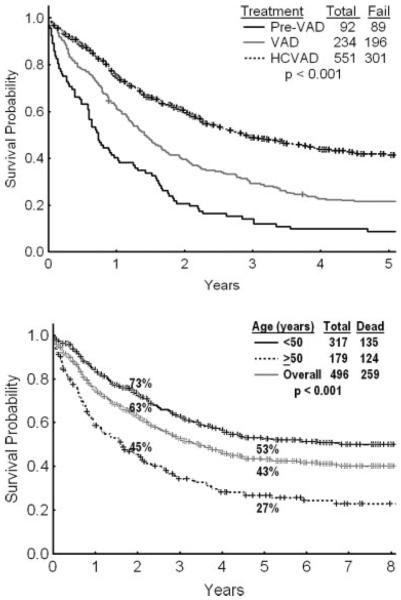
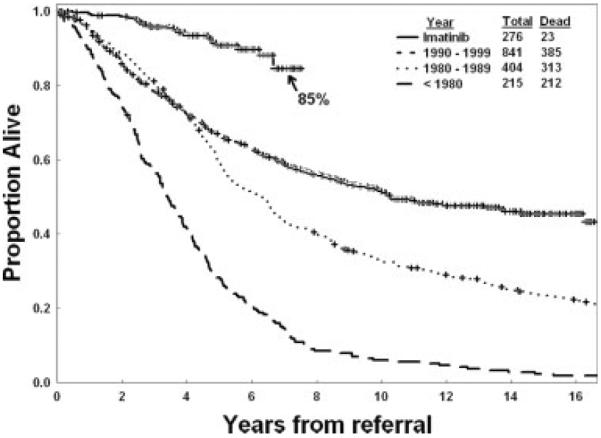
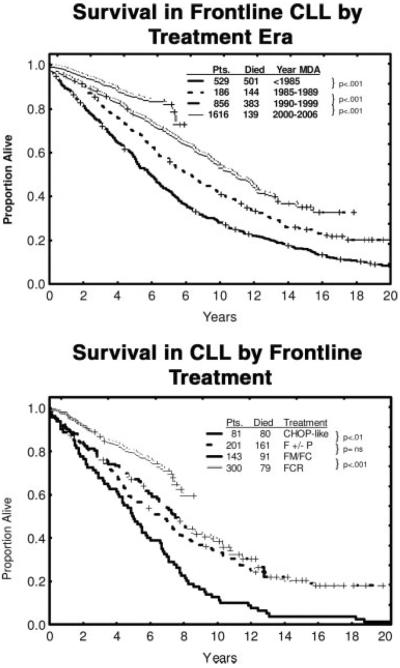
Major therapeutic progress has been accomplished in leukemia and myelodysplastic syndrome (MDS) over the past 40 years, which may not be fully appreciated by the larger medical community. The objective of this review was to briefly highlight the treatment breakthroughs in leukemia and MDS. Therapeutic progress happened through better understanding of disease pathophysiologies and rational development of targeted agents, like imatinib mesylate in chronic myeloid leukemia (CML), and through astute, empirical discoveries in the clinic, like all-trans retinoic acid and arsenic trioxide in acute promyelocytic leukemia (APL) and chlorodeoxyadenosine in hairy cell leukemia (HCL). Today, the 5- to 10-year survival rates in patients with APL and HCL exceed 80%. In patients with CML, imatinib therapy has been associated with estimated 5- to 7-year survival rates from 85% to 90%. In patients with adult acute lymphocytic leukemia, modern intensive regimens have improved the 5-year survival rates from 20% up to 40%. In patients with chronic lymphocytic leukemia, chemoimmunotherapy recently produced high rates of quality responses and improved long-term outcome. In younger patients with acute myeloid leukemia (AML), the 5-year survival rates range from 40% to 50%, although elderly AML remains a therapeutic challenge. In patients with MDS, it was recently demonstrated that epigenetic therapy with hypomethylating agents improved survival. Much therapeutic progress has been witnessed in leukemia and MDS, and much more is expected to occur soon.
Figures
References
-
- Freireich EJ, Bodey G, Harris J, Hart J. First continuous infusion (12) hour Ara-C 14 patients, 6 CRs and 2 PRs. Therapy for acute granulocytic leukemia, Cancer Res. 1967;27:2573–2577. - PubMed
-
- Boiron M, Weil M, Levey D, et al. Daunorubicin in the treatment of acute myeloblastic leukemia. Lancet. 1969;1:330–333. - PubMed
-
- Ravandi F, Burnett AK, Agura ED, Kantarjian H. Progress in the treatment of acute myeloid leukemia. Cancer. 2007;110:1900–1910. - PubMed
-
- Mayer RJ, Davis RB, Schiffer CA, et al. Intensive post remission chemotherapy in adults with acute myeloid leukemia. Cancer and Leukemia Group B. N Engl J Med. 1994;331:896–903. - PubMed
-
- Weick JK, Kopecky KJ, Appelbaum FR, et al. A randomized investigation of high-dose versus standard-dose cytosine arabinoside with daunorubicin in patients with previously untreated acute myeloid leukemia: a Southwest Oncology Group study. Blood. 1996;88:2841–2851. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
