

Neurodegeneration associated with genetic defects in phospholipase A(2)
- PMID: 18799783
- PMCID: PMC2676964
- DOI: 10.1212/01.wnl.0000327094.67726.28
Neurodegeneration associated with genetic defects in phospholipase A(2)
Abstract
Objective: Mutations in the gene encoding phospholipase A(2) group VI (PLA2G6) are associated with two childhood neurologic disorders: infantile neuroaxonal dystrophy (INAD) and idiopathic neurodegeneration with brain iron accumulation (NBIA). INAD is a severe progressive psychomotor disorder in which axonal spheroids are found in brain, spinal cord, and peripheral nerves. High globus pallidus iron is an inconsistent feature of INAD; however, it is a diagnostic criterion of NBIA, which describes a clinically and genetically heterogeneous group of disorders that share this hallmark feature. We sought to delineate the clinical, radiographic, pathologic, and genetic features of disease resulting from defective phospholipase A(2).
Methods: We identified 56 patients clinically diagnosed with INAD and 23 with idiopathic NBIA and screened their DNA for PLA2G6 mutations.
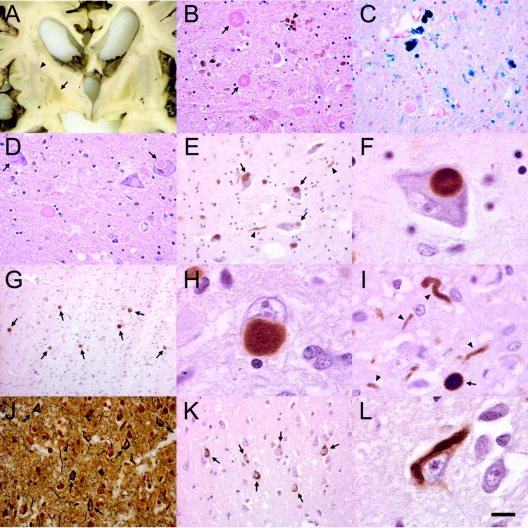
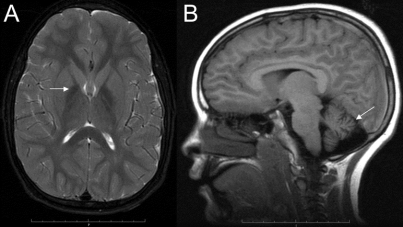
Results: Eighty percent of patients with INAD had mutations in PLA2G6, whereas mutations were found in only 20% of those with idiopathic NBIA. All patients with two null mutations had a more severe phenotype. On MRI, nearly all mutation-positive patients had cerebellar atrophy, and half showed brain iron accumulation. We observed Lewy bodies and neurofibrillary tangles in association with PLA2G6 mutations.
Conclusion: Defects in phospholipase A(2) lead to a range of phenotypes. PLA2G6 mutations are associated with nearly all cases of classic infantile neuroaxonal dystrophy but a minority of cases of idiopathic neurodegeneration with brain iron accumulation, and genotype correlates with phenotype. Cerebellar atrophy predicts which patients are likely to be mutation-positive. The neuropathologic changes that are caused by defective phospholipase A(2) suggest a shared pathogenesis with both Parkinson and Alzheimer diseases.
Figures
Comment in
-
Neurodegeneration associated with genetic defects in phospholipase A2.Neurology. 2009 Sep 8;73(10):819. doi: 10.1212/WNL.0b013e3181b2851b. Neurology. 2009. PMID: 19738181 No abstract available.
References
-
- Nardocci N, Zorzi G, Farina L, et al. Infantile neuroaxonal dystrophy: clinical spectrum and diagnostic criteria. Neurology 1999;52:1472–1478. - PubMed
-
- Farina L, Nardocci N, Bruzzone MG, et al. Infantile neuroaxonal dystrophy: neuroradiological studies in 11 patients. Neuroradiol 1999;41:376–380. - PubMed
-
- Simonati A, Trevisan C, Salviati A, Rizzuto N. Neuroaxonal dystrophy with dystonia and pallidal involvement. Neuropediatrics 1999;30:151–154. - PubMed
-
- Hayflick SJ. Pantothenate kinase-associated neurodegeneration (formerly Hallervorden-Spatz syndrome). J Neurol Sci 2003;207:106–107. - PubMed
-
- Hayflick SJ, Westaway SK, Levinson B, et al. Genetic, clinical, and radiographic delineation of Hallervorden-Spatz syndrome. N Engl J Med 2003;348:33–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical