

White matter tauopathy with globular glial inclusions: a distinct sporadic frontotemporal lobar degeneration
- PMID: 18800011
- PMCID: PMC2785030
- DOI: 10.1097/NEN.0b013e318187a80f
White matter tauopathy with globular glial inclusions: a distinct sporadic frontotemporal lobar degeneration
Abstract
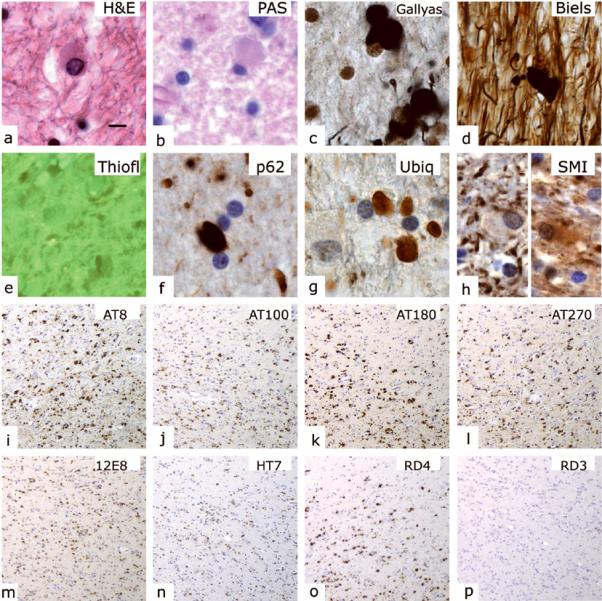
Frontotemporal lobar degenerations are a group of disorders characterized by circumscribed degeneration of the frontal and temporal lobes and diverse histopathologic features. We report clinical, neuropathologic, ultrastructural, biochemical, and genetic data on 7 individuals with a 4-repeat tauopathy characterized by the presence of globular glial inclusions (GGIs) in brain white matter. Clinical manifestations were compatible with the behavioral variant of frontotemporal dementia and included motor neuron symptoms; there was prominent neuronal loss in the frontal and temporal cortex, subiculum, and amygdala. The surrounding white matter showed abundant GGIs composed of abnormal filaments present mostly in oligodendrocytes. The severity of white matter tau abnormalities correlated with a reduction in myelin and axons and with microglial activation. Western blotting of sarkosyl-insoluble tau demonstrated the presence of 2 major tau bands of 64 and 68 kd. No mutations in the microtubule-associated protein tau gene were detected in 2 affected individuals. We propose that 4-repeat tau-immunoreactive GGIs are the neuropathologic hallmark of a distinct sporadic tauopathy with variable clinical presentations that include frontotemporal dementia and occasionally upper motor neuron disease. This type of tauopathy with GGIs expands the group of neurodegenerativedisorders in which oligodendroglial pathology predominates, beyond the synucleinopathy multiple system atrophy disorders.
Figures






References
-
- Boxer AL, Miller BL. Clinical features of frontotemporal dementia. Alzheimer Dis Assoc Disord. 2005;19(Suppl 1):S3–6. - PubMed
-
- Neary D, Snowden JS, Gustafson L, et al. Frontotemporal lobar degeneration: A consensus on clinical diagnostic criteria. Neurology. 1998;51:1546–54. - PubMed
-
- Knibb JA, Kipps CM, Hodges JR. Frontotemporal dementia. Curr Opin Neurol. 2006;19:565–71. - PubMed
-
- Goedert M, Spillantini MG. A century of Alzheimer's disease. Science. 2006;314:777–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
